
I am nearing the completion of my Youth for India fellowship journey. I thought it was a good time to reminisce and reflect on all the experiences and learning I had during the course of past 13 months of my fellowship tenure. During the fellowship programme, I worked extensively on issues pertaining to public health domain, focussing specifically on maternal and child malnutrition in the tribal regions of Palghar district in Maharashtra, India. For the purpose of my project, I was based out of Walwanda village in Jawhar block.
The following blog elucidates my fellowship project details – focus area, background, rationale, objectives, methodologies devised, interventions conducted and outcomes and impact achieved.
What was my fellowship project about?
My fellowship project was on – Social behaviour change communication (BCC) and community mobilisation (CM) to address the issue of maternal and child malnutrition in Palghar district, Maharashtra.
My project was broadly aimed at developing community-based malnutrition awareness interventions, that is, providing health awareness to the tribal village residents via nutrition-sensitive awareness, community mobilisation and food and nutritional security; conducting awareness sessions and campaigns focussing on vulnerable sections at the village and household level; and providing health promotion and health literacy at the tribal school targeting adolescent girls and boys.
Further, the focus group included mothers, pregnant and lactating women (PLW), newborn, children (under the age of 5) and adolescents. The target group at the village and household level were children with severe acute malnutrition (SAM) and adolescent school children studying in standard 8th and 9th, at the school level.
Why ‘malnutrition’ was the primary focus area of my fellowship project?
The National Family Health Survey (NFHS-4) 2015-16 revealed that 83,000 children, below the age of six years, were found to be severely underweight in the Maharashtra. In addition to this, the National Human Rights Commission had sent a notice to the Maharashtra government over 600 malnutrition deaths that were reported from the tribal belt of Palghar in a year.
Malnutrition is a multi-dimensional and an inter-generational phenomenon. The vicious cycle of malnutrition leads to health crisis and is no less than an epidemic. There was an urgent and persistent requirement to address the critical health issue of malnutrition plaguing the tribal population in Jawhar.
The preliminary stakeholder meetings held with including, inter alia, the primary health centre and village health sub-centre officials, Anganwadi workers (AWW), Accredited Social Health Activists (ASHA), Auxiliary Midwives (ANM), women self-help groups (SHGs), community resource personnel (CRP), the village community, school children, adolescent girls and boys, the Gram Panchayat (GP) Samiti officials and Gram Sewaks, Gram Panchayat leader (sarpanch), the Panchayat members and the local NGOs, all pointed towards the major health concern of malnutrition in Jawhar.
Malnutrition, by far, has been the primary cause of deaths among children aged 0-5 years. Lack of proper nutrition, early marriages, frequent births, high fertility rate and a lack of proper birth spacing has led to widespread anaemia, related diseases and worsening health conditions among the pregnant and lactating women. This has further resulted in exacerbation of the maternal mortality and child mortality rates in Jawhar.
Factors such as early marriage, seasonal migration and meal intake were some of the factors that featured high above, amongst rest of the factors that also contributed to poor nutrition among children, adolescent girls and mothers. Other factors that have led to abysmal health profile of people in the tribal villages is lack of awareness of institutional deliveries (home deliveries carried out by the inexperienced traditional birth attendants due to un-affordability and inaccessibility to health care facilities), lack of both antenatal and postnatal care, cultural barriers and superstitions, among others.
Though, the conventional belief is that malnutrition is caused due to lack of nutrition or nutritional deficiencies of macronutrients and micronutrients. However, my understanding is that other non-conventional factors (in addition to the factors listed above) such as poor sanitation and hygiene, poor health, poverty, unemployment and poor environmental health conditions are equally vital and critical factors contributing to the menace of malnutrition in Jawhar, Palghar.
Thus, my project intervention strategies focussed on nutrition-sensitive interventions rather than only nutrition-specific interventions.
What were the objectives of my fellowship project?
The project objectives were formulated taking into account the most vulnerable sections of the tribal village, that is, mothers, pregnant and lactating women and children (age 0-5 years). The target group was a) village community and households (with severely/moderately acute malnourished children) and b) Tribal residential school (adolescent school children studying in standard 8th and 9th).
My project was conceptualised on three key pillars –
- As the foundation of nutrition programme and primary healthcare of the country’s health ecosystem, especially rural areas, the Anganwadi centres provided an effective mechanism for improving health outcomes through community-based and participatory behaviour change communication.
- Anganwadi workers and Accredited Social Health Activists could effectively mobilise members of the village community and interface with various actors and institutions to activate the public health system and respond to the needs of the most vulnerable sections of the society, that is, mothers, PLW and children under the age of 5.
- Schools, specifically tribal residential schools (ashram shalas) could effectively form the base for health information, education and communication and preventive and promotive healthcare interventions targeting adolescent children.
The dual aims of my project were to: a) mitigate the extent and severity of malnutrition among mothers, PLW and children under the age of 5 via behaviour change communication and community mobilisation; and b) ensure information and knowledge dissemination, improve health and hygiene literacy and increase the awareness levels about malnutrition and malnutrition prevention among adolescent children via interpersonal communication, among others.
In essence, the motive of my project was to address the issue of malnutrition with the following approaches viz. social behaviour change communication; information, education and communication; interpersonal communication; and community mobilisation. The project entailed both qualitative and quantitative analyses of the multiple conventional and non-conventional factors that directly or indirectly result in maternal, newborn and child malnutrition.
What was my approach to address the malnutrition issue?
The methodology devised to conduct planned interventions and impact assessment of the project was as follows –
- Institutional and stakeholder mapping – Preliminary stakeholder meetings and interviews were conducted during October 2016 – December 2016.
- Community needs assessment – The local needs assessment of the village community indicated that malnutrition (due to poor nutrition, poor health and poor living conditions) was the primary reason behind high maternal mortality and child mortality in the village. The community needs assessment was completed and baseline surveys were conducted simultaneously during the months of October 2016 – January 2017.
- Conducting baseline surveys (pre-intervention surveys at the village, households and the school) – The baseline survey conducted was based on nutrition-sensitive factor analysis. The factor analysis pertained to the following factors a) biological factors; b) socio-cultural factors; c) socio-demographic factors; d) socio-economic factors; e) environmental factors; and f) behavioural factors. The pre-intervention (preliminary) baseline surveys were conducted during November 2016 – January 2017, at the village/households and the tribal school. The findings of the baseline surveys are mentioned below.
- Designing project structure at the school and village and household level – The project structure was finalised in the month of January 2017.
- Implementing project interventions based on the project structure – The project interventions were conducted at the target village, households and school. The interventions were conducted throughout the tenure of the fellowship project, that is, during January 2017 – September 2017.
- Impact assessment of project interventions at the village, household and school – The project impact assessment was categorised into – (i) Nutrition-sensitive interventions assessment (nutrition-sensitive factor analysis) and Nutrition-specific interventions assessment (nutrition garden initiative). The monitoring and evaluation was completed during the month of September 2017.
The Baseline Survey – Findings
A comprehensive approach was devised to address the issue of malnutrition among the target group that ensures community ownership.
Baseline surveys were conducted at the target village (Walwanda village), village households and the school (Walwanda Tribal High School, a tribal residential school or ashram shala). These surveys formed the basis for designing project interventions and activities at the school, household and village level.
Village Level – Baseline Survey
Baseline survey conducted at the Walwanda village suggested that there are approximately 200 households. The population comprises of c.320 males and c.300 females. The total number of children (0-5 years old) was c.80. Out of this, approximately 55 children were enrolled at the village Anganwadi centre. The SAM children (0-5 years old) in the village were 12 in number, with 3 male SAM cases, 7 female SAM cases and 2 female MAM cases.
Household Level – Baseline Survey
Baseline survey at the household level was conducted for a population size of 117 households. The sample size was 12 households (that is, the target group for the project intervention). The aim of the project was to focus only on the target group of 12 households. This is due to the fact that baseline survey data suggested these 12 households had children (under the age of 5) that were SAM (severe acute malnourished) or MAM (moderate acute malnourished), as per factors such as body weight, height, mid-upper arm circumference and body mass index calculation prescribed by the World Health Organisation. On an average, each household had 6 members with at least 1 and at most 3 children severely malnourished. The baseline survey conducted was based on nutrition-sensitive factor analysis. The factor analysis pertained to the following factors viz. a) biological factors; b) socio-cultural factors; c) socio-demographic factors; d) socio-economic factors; e) environmental factors; and f) behavioural factors.
Following were some critical facts and findings of the factor analysis –
- There were 10 children that were severe acute malnourished and 2 children that were moderate acute malnourished. That is, 12 children were stunted (low height for age), wasted (low weight for height) or undernourished (low weight for age) and thus categorised as SAM/MAM cases accordingly.
- Further, the data points studied to ascertain the extent of malnourishment was based on weight, height, Body Mass Index (BMI) and mid-upper arm circumference.
- As far as mothers were concerned, 3 mothers were underweight, 3 were overweight and 6 had normal weight (per BMI definition prescribed by the WHO).
- Birth-spacing was found to be normal. That is, on average 2 years.
- Out of the 12 households surveyed, 5 households were landless. The remaining households had farming land anywhere between 1 – 2 acres in area.
- Half of the village households did not have a toilet constructed at home.
Tribal Residential School – Baseline Survey
A baseline survey was conducted at the Walwanda Tribal High School in Walwanda village, Jawhar. For the purpose of analysing the outcomes and impact of the proposed project interventions on health literacy, health promotion and awareness, two surveys were conducted – pre-intervention and post-intervention.
The target group for the school project intervention was students of the school studying in the 8th and 9th standard.
Pre-intervention survey statistics: students having awareness about balanced diet (21%), hygiene (personal, food and environment) stood at 47% students, waste management (50%), child marriage (44%), Anaemia (15%) and importance of micronutrients, specifically Vitamin A (15%).
What were my project interventions?
Two-tiered project interventions were conducted, that is, one at the village and household level and the second at the school level. Broadly, the project interventions were categorised as nutrition-specific and nutrition-sensitive. Some of the vital interventions that I conducted are as follows –
Village and Household – Interventions
I. ‘Swasthya Samwad’
This intervention was based on providing health promotion and education with a specific focus on spreading awareness about malnutrition and its implications. This was done through community engagement, participation and mobilisation via Anganwadi centre in the village. The target group, that is, the SAM households was the primary focus of this intervention.
A comprehensive BCC approach (utilising all communication channels such as posters, banners, hand bills and leaflets, pamphlets, among others) was devised to disseminate vital knowledge among the households, specifically and the village community, in general.
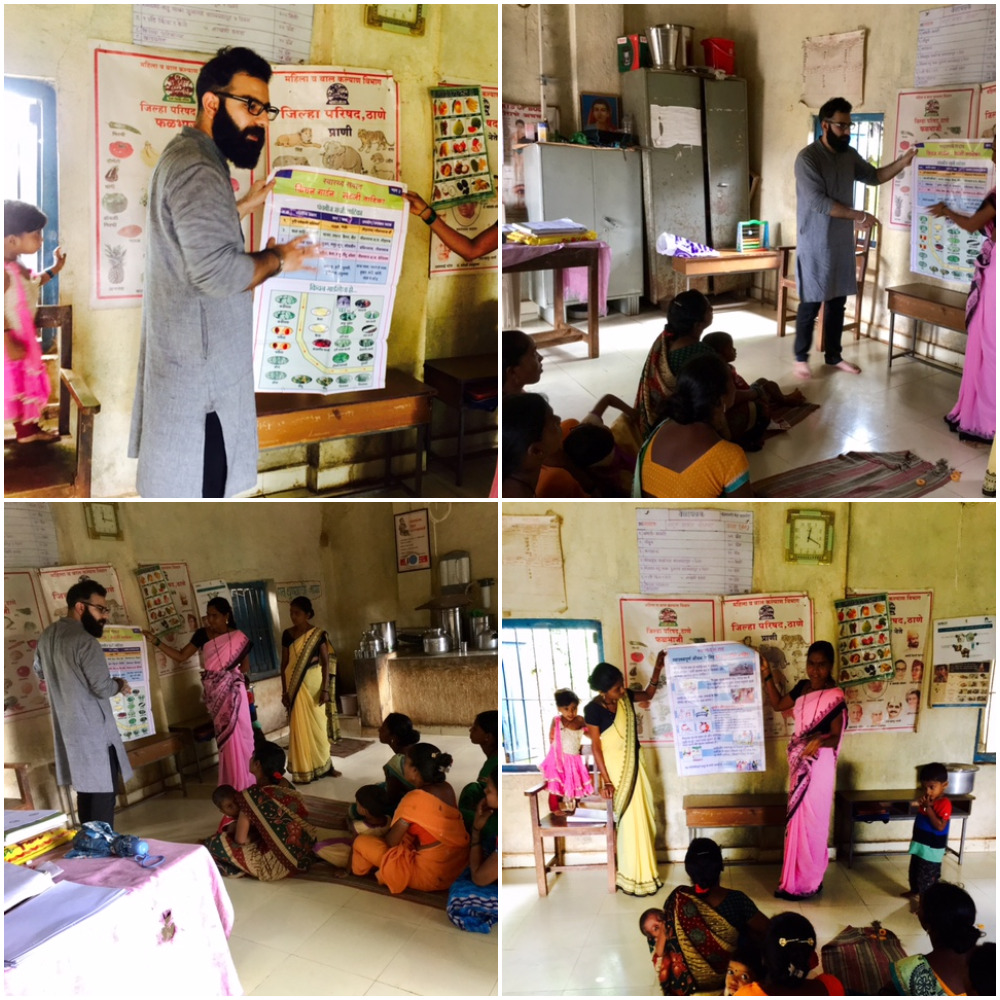
The main purpose of this intervention was to achieve higher awareness and health literacy levels among the target group, that is, ‘at-risk’ SAM households. Weekly health communication sessions (Swasthya Samwad) were carried out at the village AWC with the help of AWWs.
II. Perennial Nutrition Garden
This intervention was carried out in collaboration with the partner NGO BAIF and the village community resource person. The nutrition garden concept involved procurement ad distribution of seeds of perennial food crops/vegetables such as lady finger, spinach, among others.
Following activities were undertaken with respect to this intervention –
- Procurement of seed packets from NGO BAIF
- Distribution of vegetable seed packets among:
- SAM households; and
- Anganwadi centre

Furthermore, the SAM households were mobilised to set up nutrition gardens at their household/farmland.

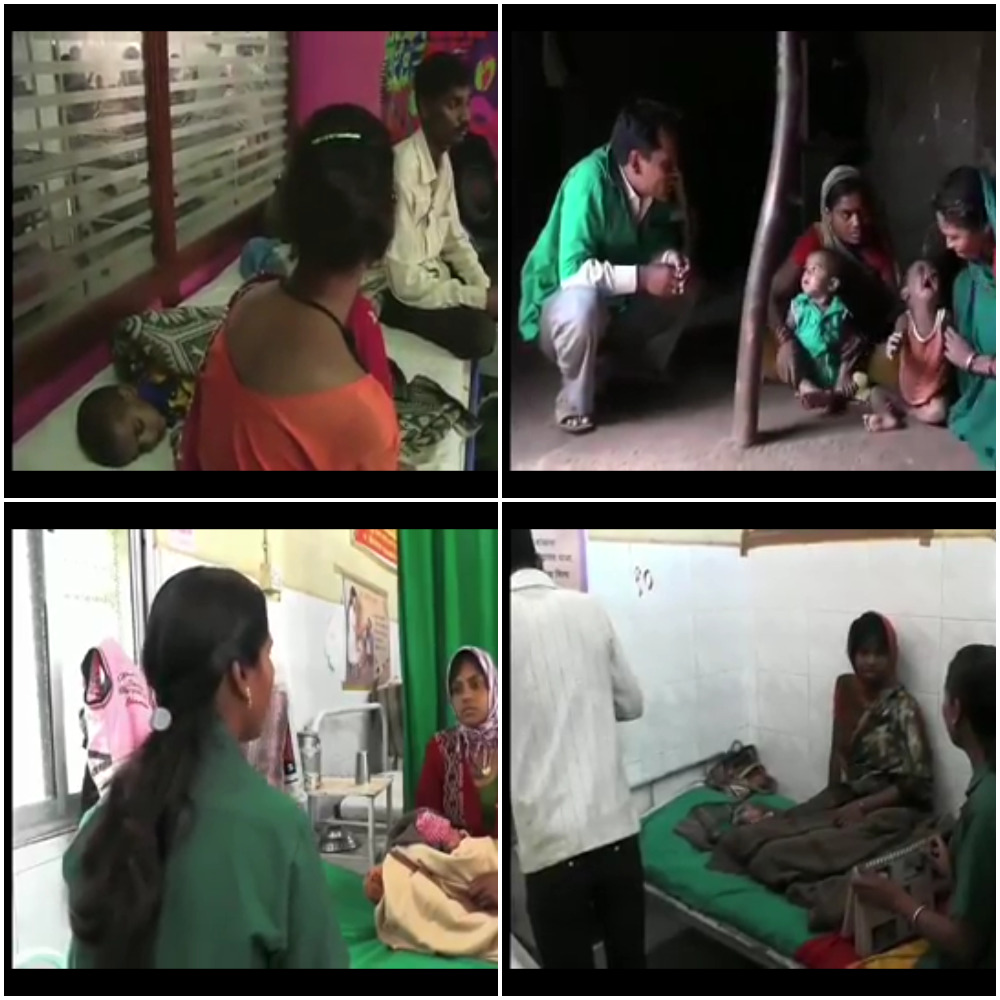
III. Health Awareness Campaigns
Various health awareness campaigns were conducted at regular intervals in collaboration with the village health sub-centre and the Anganwadi centre. The health campaigns comprised of conducting general health check-up camps, immunisation camps, awareness about mobile medical units and medicine centres and awareness on environmental health (open defecation, sanitation and general hygiene practices).
In this intervention, the primary focus was to provide the target group essential knowledge about overall good health practices to address the malnutrition issue.

IV. Traditional Healthcare Awareness
Traditional medicine is critical and has contributed tremendously to the healthcare of both the mother and the child in tribal regions. Jawhar block in Palghar district is a tribal block having rich biodiversity, especially rice varieties having specific characteristics and uses. But during the last two decades or so there has been a gradual loss of practical knowledge about traditional medicine and healing practices in the tribal regions, during the past couple of decades. This has resulted in poor health status of the most vulnerable sections of the tribal population.
In this intervention, the tribal farmers were encouraged to cultivate diverse rice varieties for purposes such as food security, instant energy provision during peak workload and medicinal use. Further, various ongoing studies conducted by the NGOs such as BAIF Development Research Foundation in different tribal belts across Maharashtra found a number of rice varieties having specific medicinal properties and uses. For instance, one rice variety called ‘Mahadi’ has multiple health benefits; one of them is to cure weakness in women post pregnancy. Other rice varieties include ‘Rajghudya’ and ‘Kali Kudai’ (used to increase breast milk in lactating women); ‘Kali Khadsi’ (for child’s growth and nutrition); ‘Kasbai’ (used for nebulisation, which gives instant relief from cough) and ‘Dangi’ (used for instant energy boost), among others.
The main purpose of this intervention was to utilise the wonderful diversity of rice and form the basis of a nutritious and secure diet for the vulnerable groups of the tribal population, that is, mothers, pregnant and lactating women and children (under the age of 5) via knowledge dissemination through face-to-face interactions with the tribal farmers.
[Also read: https://ankurchhabrablog.wordpress.com/2017/08/17/traditional-healing-practices-implications-for-healthcare/]
School – Interventions
At the school level, focussed health literacy and health promotion sessions were undertaken at the Walwanda Tribal High School. The details of the project interventions and activities (nutrition-sensitive) are mentioned below.
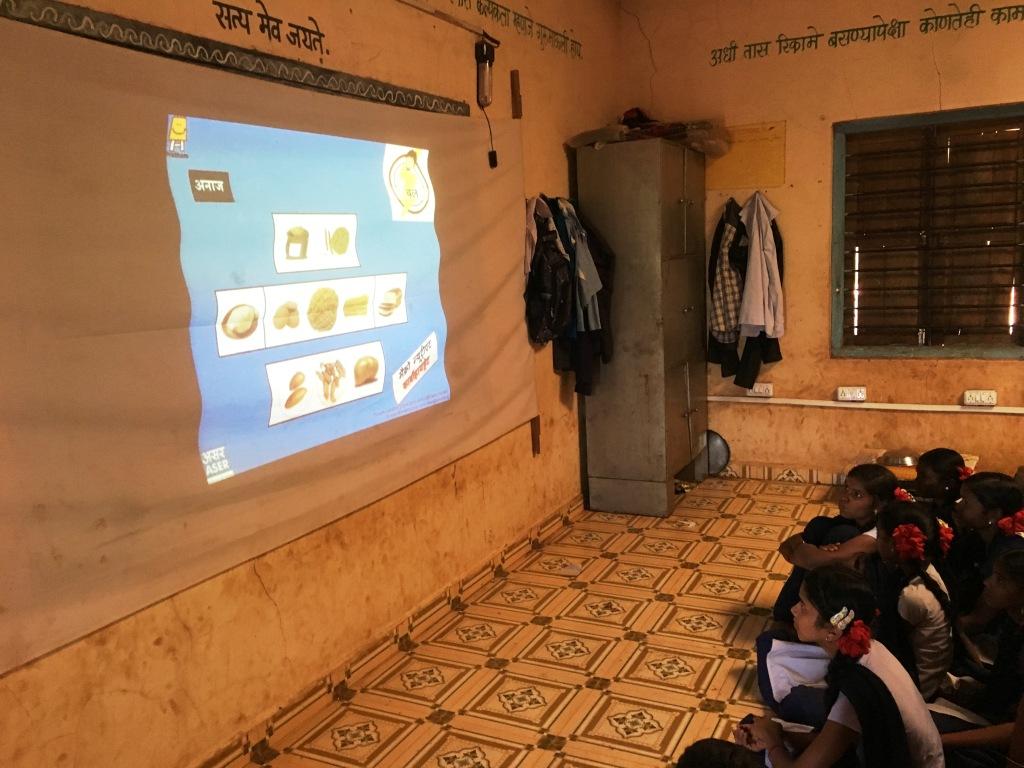
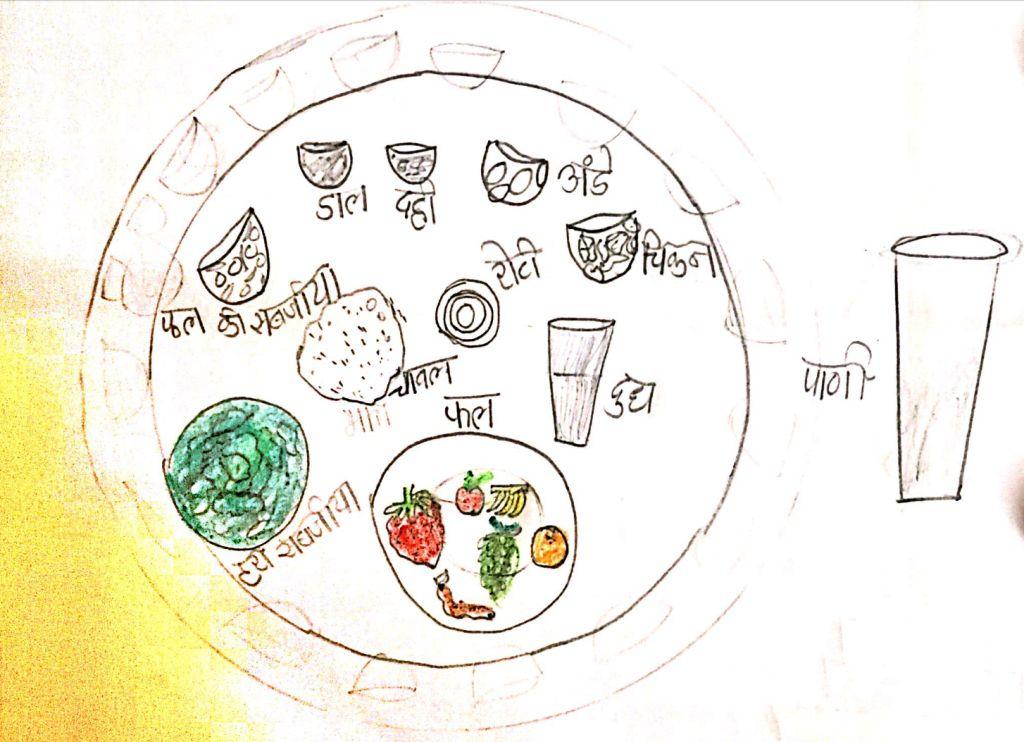
I. Food, Nutrition and Balanced Diet
The main objective of this health training module was to impart knowledge about the food types, food uses (i.e. strength, growth and immunity), importance of micronutrients (i.e. Vitamin A, Iodine, Iron, etc.), food hygiene (i.e. washing raw vegetables and eating properly cooked food), importance of exclusive breastfeeding for six months and balanced diet.
Specific focus was given to awareness on micronutrient deficiency and balanced diet. These two factors were critical from the stand point of malnutrition.
A balanced diet contains foods that provide adequate amounts of carbohydrates, fat, protein, minerals and vitamins, which help the body to grow, develop and stay healthy.
Students were encouraged to adopt a balanced diet and healthy eating practices. For this purpose, various activities and creative learning techniques were devised to spread awareness about food and nutrition.
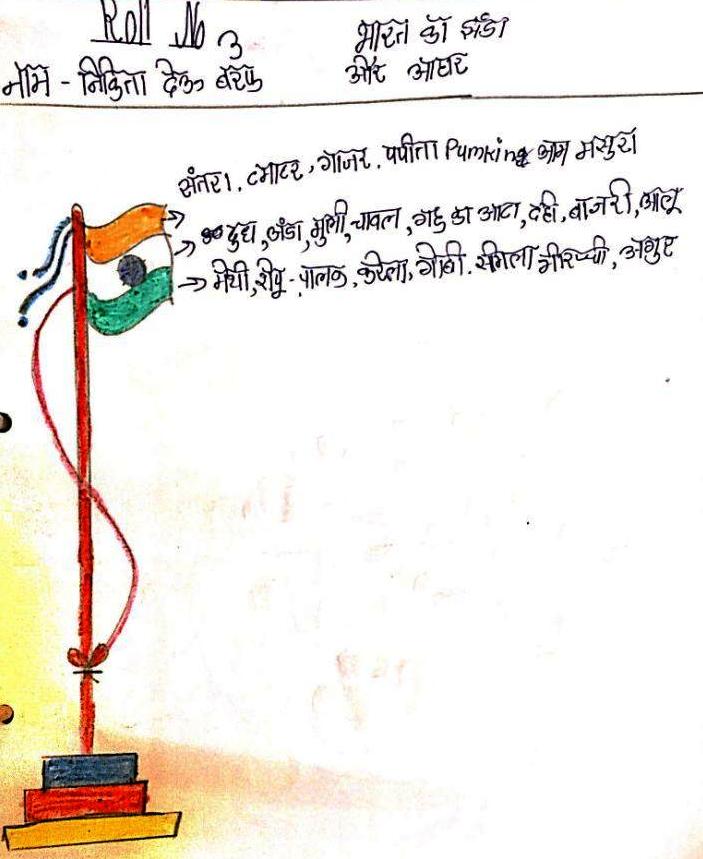
Here, the children were educated about the importance of food and nutritious food items and inter-linked with colours of the Indian national flag (i.e. saffron, white and green).
In addition to the above, the students were introduced to the concept of BMI and its calculation method (in order to calculate their own BMI regularly). Further, health education material (in collaboration with NGO Pratham) was distributed among the target group
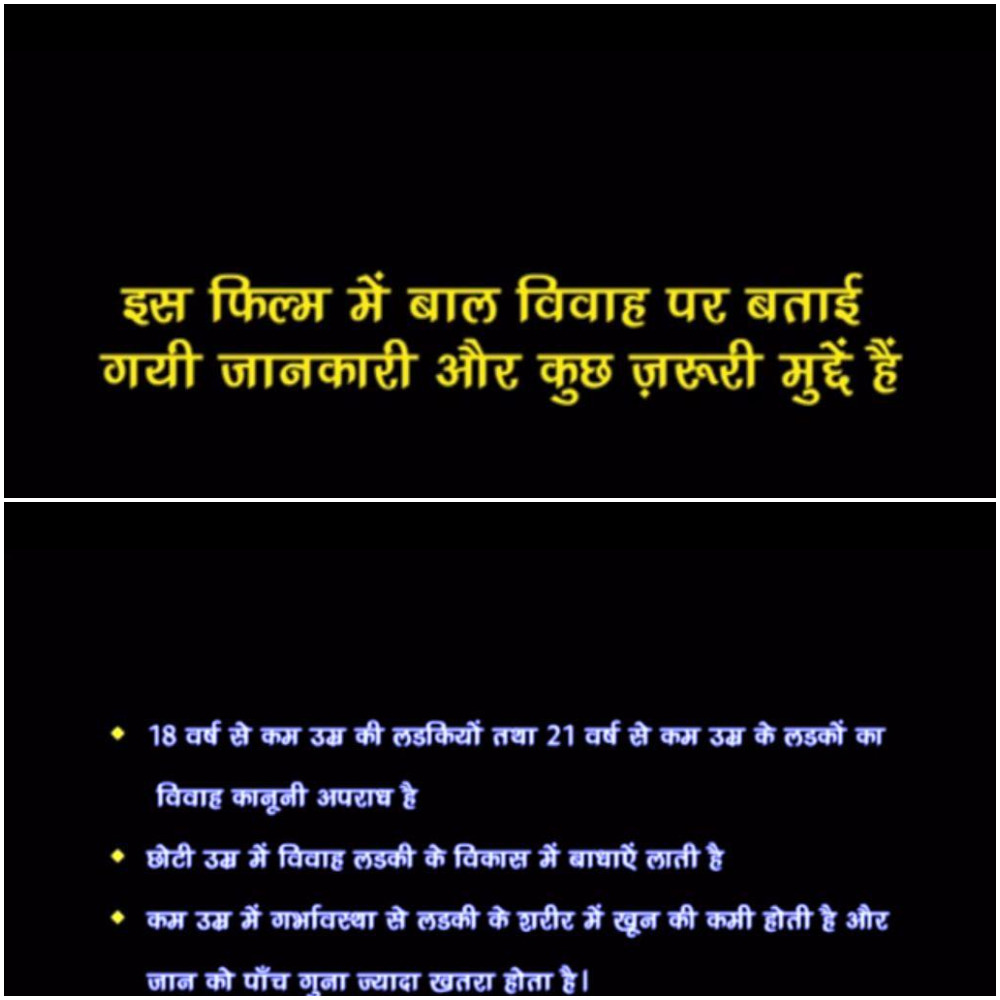
II. Girl Education
To put things in perspective regarding the importance of girl education, UNESCO reported that if all women had a primary education, 1.7 million children would be saved from stunting from malnutrition. If all women had a secondary education, 12 million children would be saved from stunting from malnutrition. Girls with higher levels of education are less likely to have children at an early age. 10% fewer girls would become pregnant under 17 years in sub-Saharan Africa and South and West Asia if they all had a primary education. Almost 60% fewer girls would become pregnant under 17 years in sub-Saharan Africa and South and West Asia if they all had a secondary education.
Further, girls with higher levels of education are less likely to get married at an early age. If all girls had a primary education, there would be 14% fewer child marriages. If all girls had a secondary education, there would be two-thirds fewer child marriages.
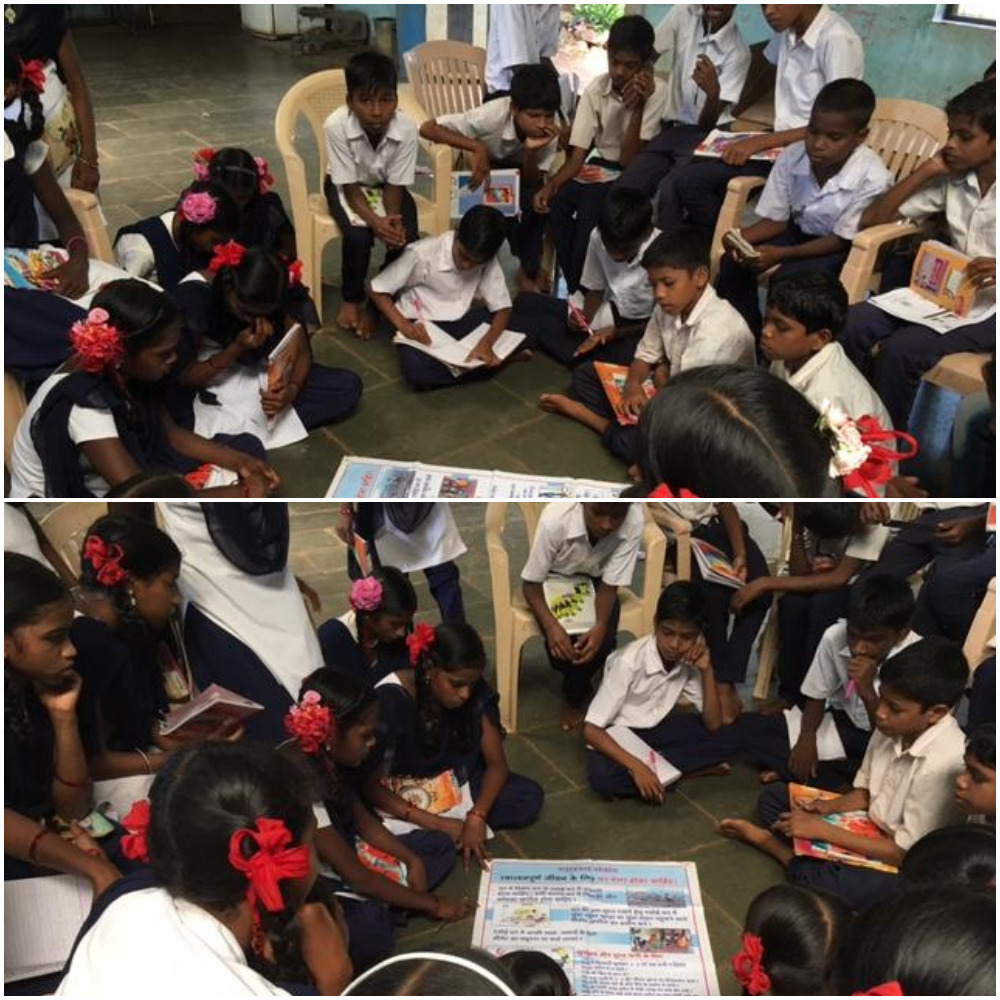
In this intervention, activities centred on class discussions and showcase of films and educational documentaries.

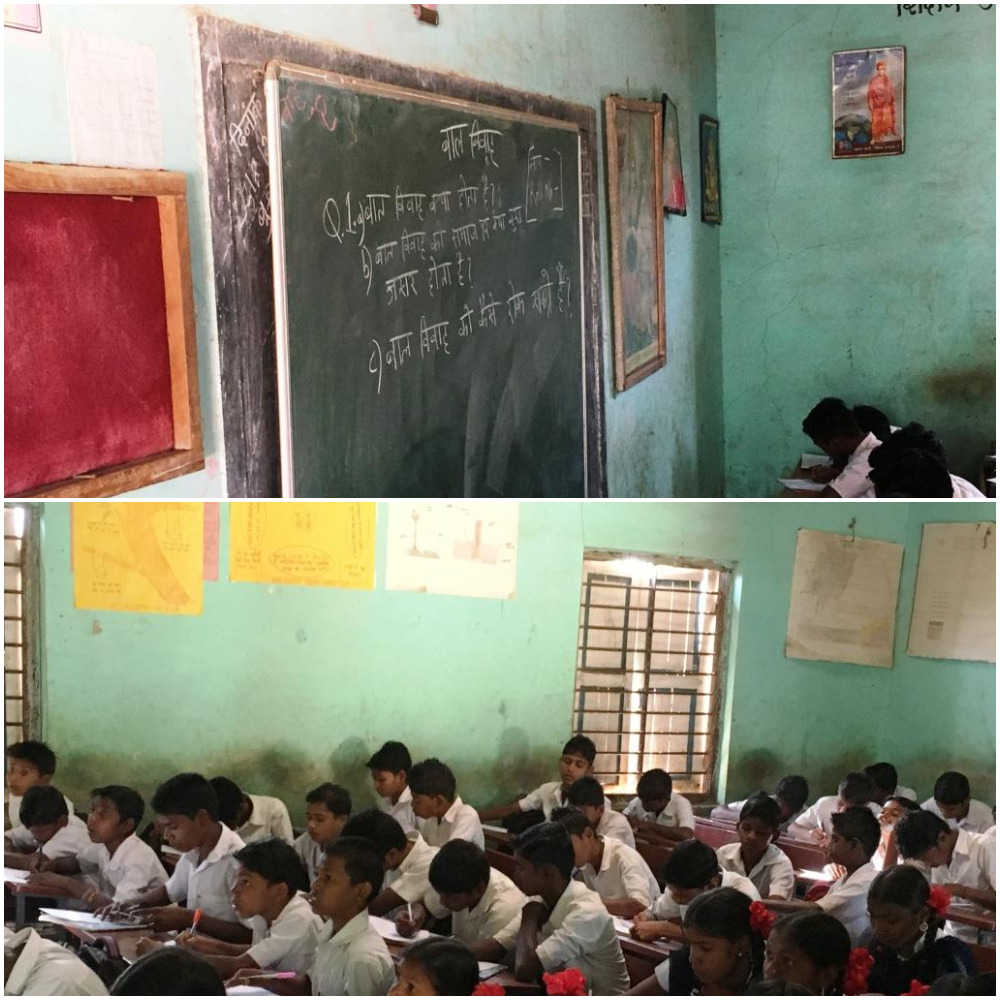
III. Child Marriage
In this intervention, activities centred on class discussions and showcase of issue based film on child marriage.
IV. Water, Sanitation and Hygiene (WASH)
There is a strong link between the high rates of child malnutrition in India and the country’s poor sanitation. The WHO estimates that 50 percent of malnutrition is associated with repeated diarrhoea or intestinal worm infections from unsafe water or poor sanitation or hygiene.
Stunting can stem from enteropathy, a chronic illness caused by inflammation that keeps the body from absorbing calories and nutrients. Children who are exposed to open defecation or who don’t have a clean water supply may ingest bacteria, viruses, fungi, or parasites that cause intestinal infection; chronic inflammation in a child’s gastrointestinal track is linked to stunting and anaemia, and puts children at risk for poor early childhood development.
The interventions that were conducted in this module were class discussions, essay-writing, awareness on hand-washing, drinking water, open defecation, waste management, among others.


V. Malnutrition Awareness
Following interventions were planned and activities conducted for spreading focussed awareness about malnutrition targeting school children.
Class Discussions on Malnutrition Awareness

Animation film on malnutrition awareness

Anaemia Awareness – Adolescent Girls

Malnutrition Board Game
As a last activity in this module, a board game was designed for providing comprehensive health and hygiene awareness to counter the issue of malnutrition. The board game was designed to ensure lasting positive impact on health education and health promotion among school children and adolescent girls, through fun and an interactive learning experience. Further, the board game was adopted very well by the school management and school students and thus was made part of the school curriculum.
In addition to the aforementioned interventions, various health awareness sessions were conducted to provide awareness about importance of immunisation, deworming, among others. School students were also taught how to calculate their BMI.
Further, health education cards were designed for children to learn specifically about the links between food and malnutrition.
Health Promotion Events
- ‘Swachh Gaon Abhiyan’
Various village and school sanitation events were conducted regularly to instil the importance of critical facets of environmental health viz. hygiene, cleanliness, waste management, among others.
- ‘Malnutrition Free India’
‘Malnutrition Free India’ event was conducted in August 2017 during India’s 71st Independence Day. The village community, including school children were mobilised to get their health check-up done. The event was conducted in collaboration with the Savali Charitable Trust and village health sub-centre in Walwanda village.

- ‘Train the Trainer’
After the health interventions to provide malnutrition awareness, the selected teachers were given the training on healthy practices and malnutrition. This was done to ensure continuity and sustainability of the project post completion of the fellowship.
- ‘Student Health Ambassador’
Two student health ambassadors from standard 8th of the Tribal High School were selected (based on student elections) to conduct training sessions for the next incoming batch of students. Further, the ‘Health Ambassador’ would conduct health promotion activities with the incoming batch of students, mobilise his/her village community and also take responsibility and ownership of managing and maintaining the resources (such as the training modules, health education material, malnutrition board game, etc.), under the supervision of school teachers and the Principal.
What was the impact of my fellowship project?
The quantitative and qualitative impact assessment results were as follows –
Village/Household Level – Impact Highlights
- 7 out 12 SAM children were categorized as ‘Normal’ (as per height)
- 1 child transitioned from ‘MAM’ category to ‘Normal’ category
- Weight – apart from 3 children, every child gained weight on an average of 0.6 kg
- Height – apart from 2 children, every child gained height on an average of 5cm
- MUAC – An average of 0.4 cm increase in MUAC for half of the children under observation
School Level – Impact Highlights
Average awareness levels –
- Importance of Balanced Diet – 100% of the class
- Hygiene (personal, food and environment) – 98% of the class
- Waste management (94%), child marriage (74%), Anaemia (75%) and importance of micronutrients, specifically Iodine (96%) and Vitamin A (74%) in the diet
- General awareness levels about malnutrition shot up to 89% (post-intervention) from 48% (pre-intervention)
Learning – The Way Forward
Separating out the impact of interventions aiming to prevent malnutrition and those that specifically target SAM might not be possible. Nevertheless, it is important to keep in mind that there are some populations that are particularly vulnerable to acute malnutrition. Programmes aiming to prevent malnutrition in these populations, therefore, need to be a mix of both nutrition-specific interventions to address acute malnutrition, as well as work synergistically with other nutrition-sensitive activities to tackle the underlying causes and reduce future vulnerability.
Health promotion, BCC and CM strategies alone could not solve all the issues impacting community health. Even if the community is fully motivated and willing to change, if the physical possibilities for that positive change are not present, no change will occur. Behavioural change takes place more easily and rapidly when target groups, however small, become involved in analysing information, discussing its relevance to their particular situation, internalising it and making decisions to take action. Any attempt to make communication a part of development and enable people to change their behaviour depends on democratic practices among the decision makers and facilitators.
Promoting positive social behavioural change is a complex process requiring a thorough understanding of what motivates people to adopt or resist new behaviours. BCC and CM approaches recognised that presenting facts alone does not guarantee behavioural change. Individuals are greatly influenced not only by their own knowledge about issues but also by social pressures exerted by their peers and the larger community including cultural and societal norms and policies. BCC strategies were therefore designed to accommodate the stage of behaviour adoption of an individual and to impart knowledge and skills and provide psychosocial support that individuals need to initiate and sustain change at every stage of BCC process.
Conclusion
The primary focus of this project was both nutrition-specific and nutrition-sensitive factors. As mentioned in the above sections, malnutrition is a multi-dimensional and an inter-generational issue. Rising malnutrition is not only a health crisis but also a ticking economic bomb.
In summary, it was noted that a combination of nutrition-specific and nutrition-sensitive strategies is an effective approach to prevent undernutrition. Post-evaluation of the project interventions concluded that nutrition-sensitive programmes can help scale up nutrition-specific interventions and create a stimulating environment in which young children can grow and develop to their full potential.
Furthermore, post-evaluation of the interventions and project objectives and aims proved that the project was successful in providing health awareness to the tribal village residents. The project was successful in both mitigating the extent and severity of malnutrition among mothers, pregnant and lactating women and children under the age of 5 via behaviour change communication and community mobilisation. The project ensured formal health information and knowledge dissemination and improved health and hygiene literacy and increased the awareness levels for malnutrition and malnutrition prevention among adolescent children via interpersonal communication, among others.
Lastly, there is a lot of scope to work on a large number of factors that lead to chronic malnutrition among the vulnerable sections of the society in the most backward tribal/rural areas of our country. This could be done via formulating specific and targeted project designs and interventions to directly or indirectly address a myriad of critical conventional and non-conventional factors to curb malnutrition in the resource-poor regions of the country.
