
Malnutrition – Background
Malnutrition is an inter-generational phenomenon. The vicious cycle of malnutrition leads to health crisis and is no less than an epidemic.
Malnutrition refers to deficiencies, excesses or imbalances in a person’s intake of energy and/or nutrients. The term malnutrition encompasses two broad categories of conditions, that is, ‘undernutrition’ including stunting (low height-for-age), wasting (low weight-for-height), and underweight (low weight-for-age), and micronutrient deficiency or insufficiency (lack of important vitamins and minerals); and ‘overnutrition’ encapsulating malnourishment caused due to consuming too many calories leading to overweight/obesity (WHO, 2016). Malnutrition issue is multidimensional and multisectoral in nature. Undernourished individuals can no longer maintain natural bodily capacities, such as growth, immunity, intellectual and physical capacities, and pregnancy and lactation in women (UNICEF, 2006).
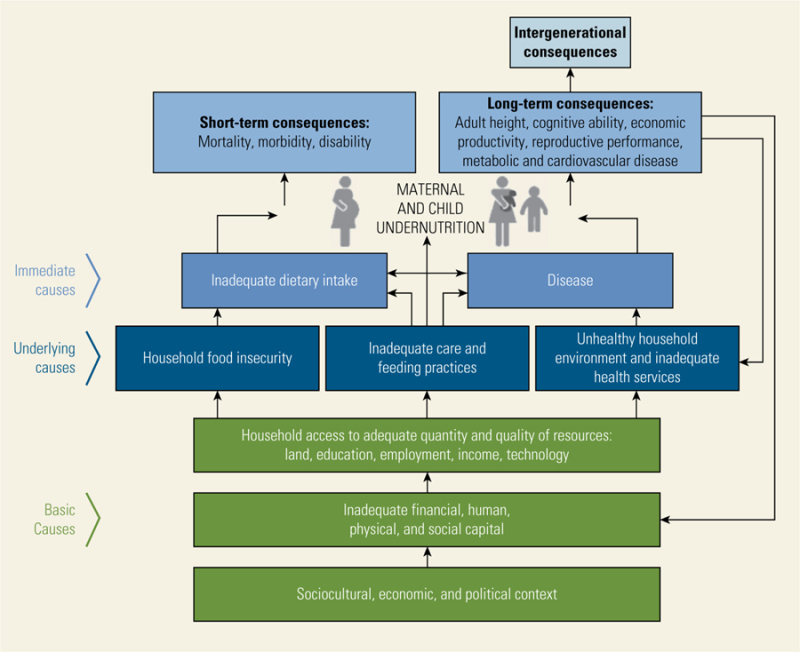
Although malnutrition can manifest in multiple ways, the pathways to prevention involves adequate maternal nutrition, optimal breastfeeding practices, access to and affordability of nutritious food for early childhood development, and a healthy environment including access to basic healthcare services and opportunities for physical activity. Combating all forms of malnutrition is one of the greatest public health challenges, in India and the world.
Undernutrition in India
The Ministry of Health and Family Welfare, Government of India, released the National Health Policy in the year 2017, which highlighted the negative impact of malnutrition on the population’s productivity, and its contribution to higher morbidity and mortality. Although India has witnessed significant progress in its battle against malnutrition over the past several years, the progress has been quite uneven, and child malnutrition rates remain high in many parts of the country.
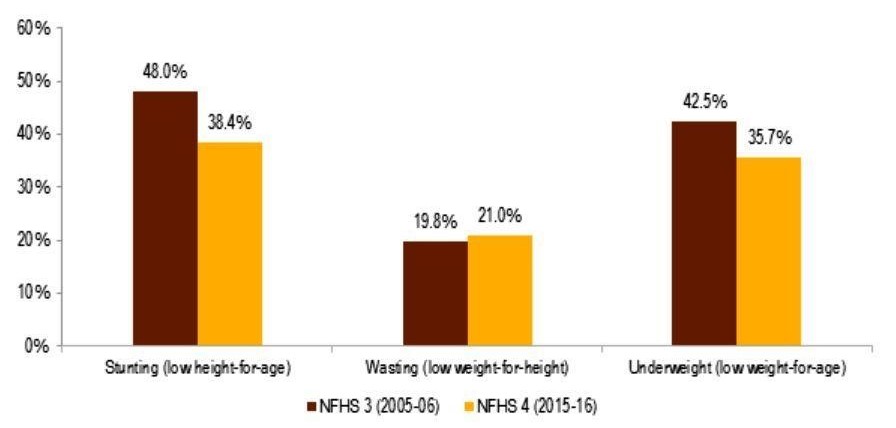
According to the National Family Health Survey (2015-16), the proportion of underweight children fell nearly 7 percent to 36 percent, while the proportion of stunted children declined nearly 10 percent to 38 percent. Despite the progress, these rates are still considerably higher than those of many low- and middle-income countries in sub-Saharan Africa.
Empirical evidence suggests that socioeconomic factors such as low income, poverty, food insecurity, maternal illiteracy, low societal status of women, poor sanitation and hygiene, and other environmental and structural factors are likely reasons for high malnutrition in India.
The multidimensional health inequities and social determinants of malnutrition have been elucidated in the subsequent sections of this article.
Social Determinants of Malnutrition – Empirical Evidence
There is considerable empirical evidence that has recognized the importance of social determinants of health (SDOH) in India. Cowling et al. (2014) extracted household and individual-level SDOH indicators from national household surveys conducted between 1990 and 2011. The study indicated air pollution, child undernutrition, unimproved sanitation, employment conditions, and gender inequality as priority SDOH issues in India. This finding is critical as the aforementioned factors have direct and/or indirect implications for malnutrition in India.
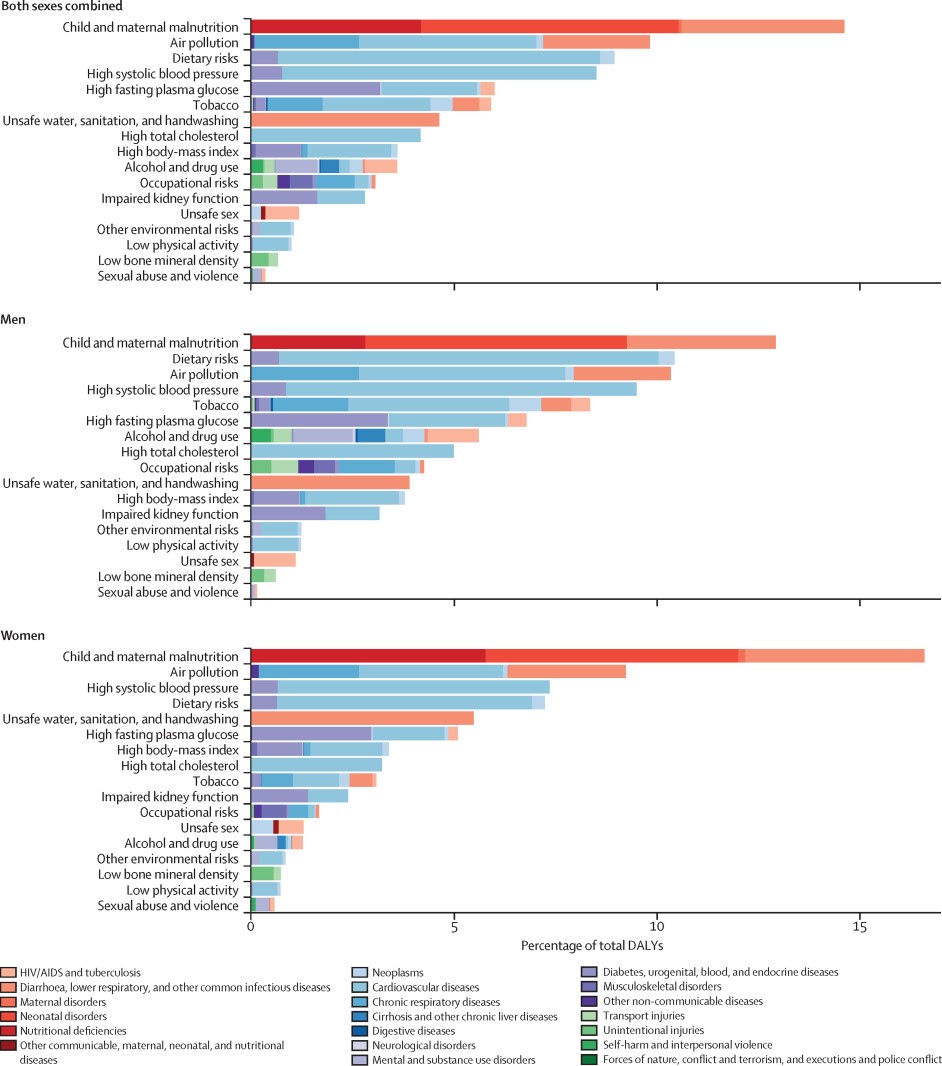
Further, the Global Burden of Disease Study estimated disease burden and risk factors to effectively improve population health in India over time. The report concluded that maternal and child malnutrition were among the leading risk factors accounting for 15% of the total disability-adjusted life-years (DALYs). The study also noted that child and maternal malnutrition and unsafe water, sanitation, and hand washing contributed more to the DALYs in women than in men. Conversely, the proportion of total DALYs due to dietary risks, high systolic blood pressure, high fasting plasma glucose, high cholesterol, and high body-mass index were found to be highest in the states that experienced high epidemiological transition level. This, in essence, explains the reason behind the co-existence of underweight and overweight, symptomatic of the ‘double burden of malnutrition‘ (DBM) in India.
Furthermore, a research study by Corsi et al. (2016) assessed the simultaneous contribution of 15 known risk factors for child chronic undernutrition in India. The study concluded that maternal stature, education, household wealth, dietary diversity, and maternal body mass index (BMI) were the top five risk factors, accounting for more than 65% of the Population Attributable Risks for child undernutrition.
Similar findings were reported by Kim et al. (2017) after assessing the relative importance of 13 risk factors such as complementary feeding, breastfeeding, feeding frequency, dietary diversity, maternal height, BMI, education, age at marriage, child vaccination, access to improved drinking source and sanitation facilities, household indoor air quality, and household wealth. India was found to have the highest prevalence of child stunting due to short maternal stature, lack of nutrition supplementation, among others.
The above research findings point towards the complex, non-linear, multi-factorial nature and scope (interplay of child, maternal, household, environmental, and socioeconomic factors) of malnutrition. Thus, it is critical to understand the multidimensional social and biological mechanisms that have resulted in abysmal child and maternal nutritional profile in India. Each of these factors has been examined in detail in the following section of this article.
Pathways to Malnutrition: Social and Biological Factors
The key social factors responsible for high malnutrition in India pertain to the socioeconomic status and inequalities, women’s status and empowerment, gender disparities, adult (maternal) literacy, environmental determinants, structural barriers, among others.
Socioeconomic Status (SES)
There is a general notion that economic growth reduces malnutrition. However, in India, evidence suggests that macroeconomic growth is not correlated with any substantial reductions in the prevalence rates of malnutrition over time.
An assessment of trends in social disparities and childhood undernutrition by Subramanyam et al. (2010, 2011) noted that the socioeconomic disparities either increased or remained constant during a time of major economic growth. The positive effect of economic growth experienced by children from socioeconomically privileged households, with better educated mothers was found to be greater than disadvantaged children. Kumar et al. (2015) examined the patterns in socioeconomic inequality in urban India and noted a decline in the prevalence of childhood undernutrition to be higher among the affluent socioeconomic groups than among the worse-off groups. Similarly, Bharati et al. (2011) found that children with illiterate mothers, of lower age groups, or from low standard of living households are more prone to become malnourished.
Interestingly, SES also has adverse effects on the rising DBM issue in India, as reported by Gaur et al. (2013) that examined the intra-city distribution of women’s nutritional profile with a focus on slum and non-slum divide. The study found that there was a prevalence of undernutrition among slum dwellers and overnutrition among non-slum women.
Further, there is evidence linking social class and nutritional stress. Mandal et al. (2011) found a direct relationship between the social class and nutritional outcomes, that is, children belonging to lower social group were found to have lower body fat. This pattern of socioeconomic segregation is consistent with the fact that there is a larger concentration of underweight women among the low socioeconomic group and of overweight/obese women among the high socioeconomic group (Kulkarni et al. 2017). Additionally, there are other socioeconomic perspectives such as food price shocks, household income, and resource allocation that have adverse effects on dietary quality and nutritional status (Bouis et al., 2011; Borkotoky et al., 2018).
Economic prosperity alone is unlikely to reduce the burden of malnutrition in India. Addressing the broader SDOH that negatively contributes to malnutrition prevalence, especially in specific demographic subgroups such as rural young females, as identified by Siddiqui et al. (2017), is pertinent in curbing high malnutrition rates in India. This might require health policies and programs with staggered approach focusing on such lower SES populations.
Gender Disparity
In India, gender differential in the nutritional status is prevalent at all levels of income and follow a social gradient: the lower the SES, the worse the nutritional profile.
Mandal et al. (2011) explained an implicit issue of gender disparity plaguing the malnutrition issue in India. The study reported inadequate nutrition received by girl child belonging to the lower social stratum and thus a lower body fat. Among the marginalized populations like Indian tribes, women, in particular, are the worst sufferers of nutritional stress (Kshatriya & Acharya, 2016).
There have been found to be persistent gendered effects of siblings on child malnutrition for both boys and girls. Raj et al. (2015) documented that having brothers heightens girl (sisters’) risk for acute malnutrition (wasting), whereas having multiple sisters increases girl’ risk for chronic malnutrition (stunting/underweight). However, malnutrition among boys was found to be less affected by the gender of siblings.
Women’s Social Status and Empowerment
Closely linked with gender disparity is the issue of low status of women in Indian society, which hinders equitable access to nutrition. There is evidence linking higher women’ and/or maternal status within a community with positive effects on daughter’s nutritional status. Bose (2011) investigated whether differences in women’s social status, both at the individual and community levels, can explain the differential in nutritional allocation among children. The study concluded that girl child is less likely than the boy child to receive supplemental food and thus more likely to be malnourished.
Further, there is a direct positive relationship between maternal autonomy (indicated by financial and physical autonomy) and childcare. Women with higher autonomy are significantly less likely to have a stunted child (Shroff et al., 2009).
Thus, lower levels of women empowerment in India has critical ramifications leading to inter-generational cycle of malnutrition.
Sociocultural Factors
As discussed in previous sections of this article, there are a myriad of social factors that play a critical role in impacting the biological aspects with inter-generational and multi-generational effects on malnutrition. Sociocultural factors such as child marriage (a ritual still largely prevalent in backward rural areas of the country) have strong associations with morbidity and mortality of infants and children under the age of 5 in India. The risk of malnutrition is higher in young children born to mothers married as minors than among those born to women married at a majority age (Raj et al., 2010).
Further, inequitable nutritional allocation in early life for girls also has a direct negative impact on adolescent undernutrition due to sub-optimal childhood nutrition levels. Chronic undernutrition and prevailing sociocultural conditions also result in adverse adolescent pregnancy outcomes and impede post-menarcheal height growth (Rao et al., 2010). This phenomenon translates to higher child stunting rates in India.
Furthermore, domestic violence is also considered to be a major cause of malnutrition due to detrimental effects on women’s physical and psychological health. As noted by Ackerson & Subramanian (2008), the possible mechanisms for this relation include withholding of food as a form of abuse and stress-mediated influences of domestic violence on nutritional outcomes.
Environmental Factors
Malnutrition and availability of potable water and proper sanitation facilities are integral and interrelated components. As discussed earlier, although over the past decade, India’s economic growth has been remarkable – yet almost half of India’s children under the age of 5 remain stunted.
Indian children suffer from malnutrition due to recurring gastrointestinal infections (resulting from lack of sanitation rather than food insecurity). High number of diarrhoeal infections, lack of personal hygiene practices, and poor health and sanitation infrastructure further exacerbate the issue of chronic malnutrition among children (Saxton et al., 2016).
Potential of Public Nutrition Schemes
Child and maternal malnutrition continues to be the leading risk factor in India. The high present and future disease burden caused by malnutrition in women of reproductive age, pregnancy, and children under the age of 5 have led to interventions focused predominantly on these population subgroups.
In order to mitigate malnutrition and meet the United Nations Sustainable Development Goals targets by 2030, India has adopted the Newborn Action Plan focusing on 187 priority districts. Further, the Government of India program – Integrated Child Development Services, launched in 1975, has the goal to provide supplementary nutrition and health education, and other preschool childhood development services across the country. The Mid Day Meal Scheme, launched in 1995, provides free lunch to school children. The Indian Government legislated the National Food Security Act in 2013, with the objective of providing food and nutritional security through provision of subsidized food grains and focused nutritional support to women and children. The Rural Sanitation Program initially launched in 1986, and the revamped version – ‘Clean India Mission’, launched in 2014 by the current Prime Minister of India has an overarching goal to clean India and eliminate open defecation.
Despite a major focus of public health programs to address malnutrition in India for several decades now, the current trend seems to be persistent with rising anemia and DBM. Critical gaps in the current public health and social welfare schemes point towards a myopic view of the malnutrition issue. Until recently, the health interventions have largely focused on nutrition-specific interventions (like Mid-Day Meal, among others) leading to under-investments in behaviour change and nutrition-sensitive interventions. This has further led to a suboptimal level of integration of vital upstream factors and social determinants of health, including girls’ education, nutritional awareness, hygiene behaviour, family planning practices, social assistance programs, and other structural factors, in order to holistically address the problem of malnutrition in India.
Conclusion and Way Forward
This article presented evidence of the multidimensional and multi-generational nature of health inequities and social determinants of health associated with malnutrition in India.
Subramanian & Subramanyam (2015) and Joe et al. (2016) noted that a ‘support‐led’ strategy rather than simply relying on a ‘growth‐mediated’ strategy for addressing the root causes of malnutrition is the need of the hour. Going forward, there is an urgent need to combat all forms of malnutrition via nutrition-sensitive, health promotion, and social behaviour change interventions in conjunction with improvement of socioeconomic and human development indicators via provision of better nutrition, potable water, and proper sanitation for higher, positive, and tangible impact among the most vulnerable sections of the society. That said, existing public nutrition schemes in India are suboptimal; plagued with pilferage; inconstant beneficiary targeting; and poor implementation. This needs to be reversed via plugging leakages in public nutrition schemes (both in-kind and direct cash transfers) and addressing current impediments in social assistance schemes by improving beneficiary identification and targeting, that is, efficiently connecting hard-to-reach and chronically malnourished populations, especially mothers and children, with robust nutrition-related interventions.
References
Ackerson, L. K., & Subramanian, S. V. (2008). Domestic violence and chronic malnutrition among women and children in india. American Journal of Epidemiology, 167(10), 1188-1196.
Bharati, S., Pal, M., Chakrabarty, S., & Bharati, P. (2011). Trends in socioeconomic and nutritional status of children younger than 6 years in india. Asia-Pacific Journal of Public Health, 23(3), 324-340.
Borkotoky, K., Unisa, S., & Gupta, A. K. (2018). State-level dietary diversity as a contextual determinant of nutritional status of children in india: A multilevel approach. Journal of Biosocial Science, 50(1), 26-52.
Bose, S. (2011). The effect of women’s status and community on the gender differential in children’s nutrition in india. Journal of Biosocial Science, 43(5), 513-533.
Bouis, H. E., Eozenou, P., & Rahman, A. (2011). Food prices, household income, and resource allocation: Socioeconomic perspectives on their effects on dietary quality and nutritional status. Food & Nutrition Bulletin, 32(1 Suppl), S14-23.
Corsi, D. J., Mejia-Guevara, I., & Subramanian, S. V. (2016). Risk factors for chronic undernutrition among children in india: Estimating relative importance, population attributable risk and fractions. Social Science & Medicine, 157, 165-185.
Cowling, K., Dandona, R., & Dandona, L. (2014). Social determinants of health in india: Progress and inequities across states. International Journal for Equity in Health, 13, 88.
Gaur, K., Keshri, K., & Joe, W. (2013). Does living in slums or non-slums influence women’s nutritional status? evidence from indian mega-cities. Social Science & Medicine, 77, 137-146.
India State-Level Disease Burden Initiative Collaborators. (2017). Nations within a nation: Variations in epidemiological transition across the states of india, 1990-2016 in the global burden of disease study. Lancet, 390(10111), 2437-2460.
Joe, W., Rajaram, R., & Subramanian, S. V. (2016). Understanding the null-to-small association between increased macroeconomic growth and reducing child undernutrition in india: Role of development expenditures and poverty alleviation. Maternal & Child Nutrition, 12(Suppl 1), 196-209.
Kim, R., Mejia-Guevara, I., Corsi, D. J., Aguayo, V. M., & Subramanian, S. V. (2017). Relative importance of 13 correlates of child stunting in south asia: Insights from nationally representative data from afghanistan, bangladesh, india, nepal, and pakistan. Social Science & Medicine, 187, 144-154.
Kshatriya, G. K., & Acharya, S. K. (2016). Triple burden of obesity, undernutrition, and cardiovascular disease risk among indian tribes. PLoS ONE [Electronic Resource], 11(1), e0147934.
Kulkarni, V. S., Kulkarni, V. S., & Gaiha, R. (2017). “Double burden of malnutrition”: Reexamining the coexistence of undernutrition and overweight among women in india. International Journal of Health Services, 47(1), 108-133.
Kumar, A., Kumari, D., & Singh, A. (2015). Increasing socioeconomic inequality in childhood undernutrition in urban india: Trends between 1992-93, 1998-99 and 2005-06. Health Policy & Planning, 30(8), 1003-1016.
Mandal, G. C., Bose, K., & Koziel, S. (2011). Impact of social class on body fatness among rural pre-school bengalee hindu children of arambagh, west bengal, india. Homo, 62(3), 228-236.
Mandal, G. C., Bose, K., & Koziel, S. (2011). Impact of social class on body fatness among rural pre-school bengalee hindu children of arambagh, west bengal, india. Homo, 62(3), 228-236.
Ministry of Consumer Affairs Food and Public Distribution, Government of India (2013). National Food Security Act (NFSA). Retrieved from http://dfpd.nic.in/public-distribution.htm
Ministry of Health and Family Welfare, Government of India (2014, September). INAP: India Newborn Action Plan. Retrieved from https://www.newbornwhocc.org/INAP_Final.pdf
Ministry of Health and Family, Government of India (2017). National Health Policy 2017. Retrieved from https://www.nhp.gov.in/nhpfiles/national_health_policy_2017.pdf
Ministry of Health and Family, Government of India (2017, December). National Family Health Survey (NFHS-4) 2015-16. Retrieved from http://rchiips.org/nfhs/NFHS-4Reports/India.pdf
Ministry of Human Resource Development, Government of India. Mid day meal scheme. Retrieved from http://mdm.nic.in/
Ministry of Women and Child Development, Government of India. Integrated Child Development Services. Retrieved from https://icds-wcd.nic.in/
Office of the Prime Minister of India, Government of India (2014, October). Major Initiatives, Swachh Bharat Abhiyan. Retrieved from http://www.pmindia.gov.in/en/major_initiatives/swachh-bharat-abhiyan/
Press Information Bureau, Ministry of Rural Development, Government of India (2014, September 25). Government to spend about 2 lakh crore rupees for Swachh Bharat mission more than 11 crore toilets will be built in 5 years. Retrieved from http://pib.nic.in/newsite/PrintRelease.aspx?relid=110036
Raj, A., McDougal, L. P., & Silverman, J. G. (2015). Gendered effects of siblings on child malnutrition in south asia: Cross-sectional analysis of demographic and health surveys from bangladesh, india, and nepal. Maternal & Child Health Journal, 19(1), 217-226.
Raj, A., Saggurti, N., Winter, M., Labonte, A., Decker, M. R., Balaiah, D., & Silverman, J. G. (2010). The effect of maternal child marriage on morbidity and mortality of children under 5 in india: Cross sectional study of a nationally representative sample. Bmj, 340, b4258.
Rao, S., Gokhale, M., Joshi, S., & Kanade, A. (2010). Early life undernutrition and adolescent pregnancy outcome in rural india. Annals of Human Biology, 37(4), 475-487.
Saxton, J., Rath, S., Nair, N., Gope, R., Mahapatra, R., Tripathy, P., & Prost, A. (2016). Handwashing, sanitation and family planning practices are the strongest underlying determinants of child stunting in rural indigenous communities of jharkhand and odisha, eastern india: A cross-sectional study. Maternal & Child Nutrition, 12(4), 869-884.
Shroff, M., Griffiths, P., Adair, L., Suchindran, C., & Bentley, M. (2009). Maternal autonomy is inversely related to child stunting in andhra pradesh, india. Maternal & Child Nutrition, 5(1), 64-74.
Siddiqui, M. Z., & Donato, R. (2017). Undernutrition among adults in india: The significance of individual-level and contextual factors impacting on the likelihood of underweight across sub-populations. Public Health Nutrition, 20(1), 130-141.
Subramanian, S. V., & Subramanyam, M. A. (2015). Limits to economic growth: Why direct investments are needed to address child undernutrition in india. Journal of Korean Medical Science, 30(Suppl 2), S131-3.
Subramanyam, M. A., Kawachi, I., Berkman, L. F., & Subramanian, S. V. (2010). Socioeconomic inequalities in childhood undernutrition in india: Analyzing trends between 1992 and 2005. PLoS ONE [Electronic Resource], 5(6), e11392.
Subramanyam, M. A., Kawachi, I., Berkman, L. F., & Subramanian, S. V. (2011). Is economic growth associated with reduction in child undernutrition in india?. PLoS Medicine / Public Library of Science, 8(3), e1000424.
UNICEF (2006, May 4). A Report Card on Nutrition. Retrieved from https://www.unicef.org/progressforchildren/2006n4/index_undernutrition.html#note2
United Nations. Sustainable Development Goals. Retrieved from https://www.un.org/sustainabledevelopment/sustainable-development-goals/
World Health Organization (2016, July 8). What is Malnutrition?. Retrieved from http://www.who.int/features/qa/malnutrition/en/
