The health system is the backbone of healthcare service delivery. At a national level, health systems provide the foundation for health policy and legislative framework, resource allocation (financial and human), monitoring and governance mechanisms, provision of healthcare services (primary care, essential medicines, medical products and technologies, life saving vaccines, etc.), and health information systems, among others (Source: World Health Organization. (2010). Key components of a well functioning health system. Ginebra: World Health Organization).
Based on the current state of global affairs, my understanding is that the health systems are designed to deal with the aspects of healthcare delivery mentioned above, leaving out all the rest. Although the building blocks of health systems seem comprehensive, it does not ensure that these systems are completely immune to intrinsic and extrinsic risk factors. This article will explore gaps in the current global health systems – high-income countries, and low-and middle-income countries, especially humanitarian and conflict-affected settings. It will also shed light on the need to design ‘conflict-proof’ health systems for robust healthcare delivery.
There is a common notion that high-income countries have robust health systems, but this is far from the truth. For instance, the United States (U.S.) is marred by unequal and inequitable health outcomes due to disparate health sub-systems, and discriminate social determinants of health (Source: World Health Organization. (2013). Backgrounder 3: Key concepts), such as employment (Source: Goodman, N. (2015). The impact of employment on the health status and health care costs of working-age people with disabilities. Lead Center Policy Brief), income, education (Source: Hahn, R. A., & Truman, B. I. (2015). Education improves public health and promotes health equity. International journal of health services, 45(4), 657-678), crime rates, poverty, health insurance, among others. In particular, the high number of uninsured people in the U.S., make it one of the most expensive and inefficient health systems in the developed world. This certainly raises the question as to how well a developed and rich country like the U.S. is placed to provide adequate financial risk protection for poor and vulnerable populations. Furthermore, in Canada, though there is publicly funded healthcare, healthcare delivery is fragmented, leading to long wait times, and particularly poor health outcomes among First Nations communities, as a result of living in ‘third world conditions’. An example of such conditions is the national systemic failure to provide potable water, which is one of the critical factors that has led to poor health outcomes among these communities.
The above cases of healthcare system failures in high-income countries depict health disparities due to the inadequate investment in upstream factors such as primary care, social determinants of health, etc. Increased enforcement mechanisms, and enhanced focus on social and human infrastructure is as important as investments in physical infrastructure (institutions, hospitals, etc.). Global health systems need to be designed in a way that ensures health care and not only sick care. This is particularly critical in countries experiencing war and conflict.
In fragile states, the negative externalities of weak health systems are particularly gruesome. For instance, much of the conflict in Yemen is collateral damage as a result of the U.S. foreign policy. The ulterior motives and selfish interests of the U.S are an implicit factor for a weak political and health system in Yemen. Involvement of foreign governments in Yemen, and Saudi Arabia’s ‘inhumane’ foreign policy have further exacerbated the conflict, especially in the Middle East. Saudi Arabia and the United Arab Emirates have not only bombarded Yemen, but have also intentionally blockaded humanitarian aid (indirectly supported by the U.S.) from reaching millions in need. Over 14 million people (i.e. half of the country’s population) are currently on the verge of starvation. In this case, the United Nations (UN) has also failed miserably in its humanitarian response. This has had further ramifications on Yemen’s fragile health system. Yemen’s case depicts how geopolitics and foreign policy is also a determinant of national health systems. It is high time that the UN addresses this issue by revisiting international humanitarian law frameworks and ensuring those are upheld rather than just ‘managing’ the situation in Yemen and other humanitarian emergency and conflict-affected settings.
Lastly, the World Health Organization must take a lead on this and reorient health systems, both in research and practice, to counter such crises. The biggest concern is that the current understanding of health systems is limited in scope and design. What is considered essential to be part of a health system and what is excluded and on what basis? Should humanitarian law, human rights principles, and geopolitical factors be an intrinsic part of health systems?
Current social, economic, political and legal systems, especially in conflict-affected settings, do not seem to bridge the gap. This results in further paralyzing already weak health systems; increasing foreign participation and privatization; and fragile states’ overdependence on unsustainable development aid. Development aid agencies must support such states with adequate interventions that aim to support and strengthen weak healthcare systems. That said, these agencies must ensure maintenance of state sovereignty and autonomy, and sustainability of such systems in the long run. This requires investment in internal health systems strengthening human resources, as well as financial resources.
A key element of human resources is investing in women, that is, healthcare system leadership by women, women-centred health research, and gender-based medicine. These factors are pertinent to strengthen the healthcare systems in both the developing and developed world. An important facet of reorientation of health systems is to incorporate gender equitable norms, in health and medicine research and development. In the U.S., the National Institutes of Health Revitalization Act was passed in the year 1993, however, two decades later a research study found that the proportion of minority patients enrolled in clinical trials still remains persistently low (Source: Chen Jr, M. S., Lara, P. N., Dang, J. H., Paterniti, D. A., & Kelly, K. (2014). Twenty years post‐NIH Revitalization Act: enhancing minority participation in clinical trials (EMPaCT): laying the groundwork for improving minority clinical trial accrual: renewing the case for enhancing minority participation in cancer clinical trials. Cancer, 120, 1091-1096). Further, in Canada, there is a growing concern for inclusion of racial health data. Thus, it is equally important to make the medico-legal system an intrinsic part of the health systems across the globe. Healthcare system researchers and leaders need to advocate for, and monitor adherence to health-related legislation to ensure scientific rigor via equal representation of minorities, among other vulnerable population sub-groups. Thus, doing away with gender-biased medicine and making way for gender-based medicine must be the way forward.
In conclusion, in order to close the healthcare gaps, it is pertinent to understand that the sum of parts is greater than whole. Strengthening every component of the health system, guided by the principle of ‘gender parity’ must inform future health systems’ thinking and design processes. Health systems must be of the people, by the people, and for the people.
This blog post was originally published in the University of Toronto's Global Health Magazine - Juxtaposition on April 5th, 2020
Preamble to the Constitution of the World Health Organization (WHO) as adopted by the International Health Conference held in New York in 1946 and entered into force on April 7th, 1948 (celebrated as the World Health Day) defined ‘health’ as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”. However, this conceptualization of health is not holistic, both in nature and scope. Thus, the WHO Constitution extended this definition to include the socioecological determinants of health (Source: Glanz K, Rimer BK, Viswanath K. Health Behavior: Theory, Research, and Practice. John Wiley & Sons; 2015. 512 p.) such as internal and external environmental factors and the State’s responsibility to ensure health promotion of their respective citizenry, among other factors.
The Ottawa Charter of Health Promotion also emphasized this notion via provision of adequate social, economic, political, and environmental measures to maximize the overall well-being of society (Source: Judd CM, James-hawkins L, Yzerbyt V, Kashima Y. Fundamental dimensions of social judgment: Understanding the relations between judgments of competence and warmth. Journal of Personality and Social Psychology. 2005;899–913). As a result, in general, global public health has shifted from a pathogenic health approach towards a salutogenic perspective to health of individuals, communities, and populations, especially in the recent decades (Source: Huber M, Knottnerus JA, Green L, van der Horst H, Jadad AR, Kromhout D, et al. How should we define health? BMJ. 2011 Jul 26;343:d4163). This enhanced focus on external elements related to global public health promotion is inextricably linked to the concepts of attainment of peace and prosperity.
Perhaps, an alternative definition of health could entail critical elements of creating enabling health systems and conducive social environments that allow individuals, families, and communities to not only survive but thrive in an ecosystem that affords individual and societal empowerment via health equity, equality, justice, and access to socioeconomic capital (Source: Venkatapuram SS. Health Justice: An Argument from the Capabilities Approach. John Wiley & Sons; 2013. 236 p.) pertaining to food, housing, education, employment, income, and freedoms from fear, conflict, disease, and poverty (Source: Shilton T, Sparks M, McQueen D, Lamarre M-C, Jackson S, executive committee of the International Union for Health Promotion and Education-IUHPE. Proposal for new definition of health. BMJ. 2011 Aug 23;343:d5359), regardless of age, sex, and gender.
Determinants of Health and Peace Promotion
The Ottawa Charter of Health Promotion identified peace as the foundation for good health. Johan Galtung (Source: Galtung J. A Synthetic Approach to Peace Thinking. :238.), the principal founder of the discipline of peace and conflict studies, noted that individuals require both internal and external peace emanating from individual, political, cultural, and societal harmony. Internal peace is a prerequisite for extending into the external environment, that is, family, friends, and community (Source: Galtung J. Peace by peaceful means: Peace and conflict, development and civilization. Thousand Oaks, CA, US: Sage Publications, Inc; 1996. viii, 280. (Peace by peaceful means: Peace and conflict, development and civilization)).
Further, Pathways to Peace, a United Nations (UN) designated peace messenger organization developed the peace wheel model for peacebuilding constituting eight pathways – governance, education, economics, health, science and technology, religion and spirituality, environment, and culture. These interrelated peace pathways identify and engage all stakeholders as peacebuilders, transcending national, ethnic, racial, religious, age, identity, or gender differences. These pathways are interlinked and interdependent with the health promotion principles and socioecological frameworks (Source: Glanz K, Rimer BK, Viswanath K. Health Behavior: Theory, Research, and Practice. John Wiley & Sons; 2015. 512 p.).
Furthermore, health, peace, and prosperity (economic as well as social) are critical elements for ensuring human dignity and self actualization. Goals related to peace promotion are like health promotion (Source: Middleton JD. Health promotion is peace promotion. Health Promot. 1987;2(4):341–5.), with peace promotion acting as a catalyst for achieving health promotion and vice-versa. Health promotion is a bridge to peace promotion and peace promotion leads to health promotion.
Thus, global peace and global health promotion is dependent on both intrinsic and extrinsic structural factors, that is, sociopolitical peace, sociocultural harmony, and socioeconomic prosperity.
Happiness and the idea of ‘balanced’ abundance
An implicit component to achieving worldwide health, peace, and prosperity is happiness – most importantly at individual, familial, and community levels for better physical, social, and mental health outcomes for entire populations across various stages of the human life cycle. Happiness is an equally essential component at the systemic and/or structural level of the socioecological framework, that is, environmental, policy, and societal levels. Although it is difficult to evaluate peace and happiness at any level, The Institute for Economics and Peace measures the average level of global peacefulness via The Global Peace Index. Further, The UN Sustainable Development Solutions Network measures global happiness via the annual World Happiness Report and reports the Global Happiness Index based on six variables such as income, freedom, trust, healthy life expectancy, social support, and generosity. These index measures and key indicators provide some interesting insights to analyze peace and happiness in conjunction and ascertain the enablers and barriers to global peace and happiness.
However, before delving into the analysis, it is critical to understand why happiness is the most vital performance indicator for humans. Humans are distinct from other species for having rationality, which governs thought processes. Aristotle’s Nicomachean Ethicsargues that happiness is the greatest good and the end at which all human activities and efforts aim. Most of the ends are means toward other ends, however, only happiness is an end in itself – the all-encompassing primary goal of life. This makes understanding and interpreting happiness in all visions, missions, policies, and programs related to health, peace, and prosperity especially important in the current day and age.
Based on these indices, an international comparison suggests that the Scandinavian countries such as Finland, Denmark, Norway, Iceland, among others, consistently rank better than other countries year after year. These countries tend to rank higher in all the six variables, as well as emotional measures related to overall health and well-being.
On the other hand, The United States, a global economic superpower, and a country where pursuit of happiness is embedded in the deepest layers of society, is also the country with one of the highest rates of antidepressant use in the world. Although the United States ranks higher in terms of economic indicators such as capital and income, it does not even come close to the international leader board on the list of measures that make up a happy country such as generosity, social support, freedom, and corruption.
This is the biggest valuable lesson for countries vying to be the next superpowers of the world, especially emerging economies and developing countries such as India. India was ranked at 140th place in 2019 on the Global Happiness Index, dropping seven spots since 2018 on the back of an increase in negative emotions, including higher levels of worry, sadness, and anger, especially over the past few years. Compared to this, India’s neighbour, the small country of Bhutan came in at 95th place.
Both these indices depict one thing clearly – the country that grows (both economically and socially) together equally and equitably, stays together peacefully and happily. This simplistic idea and a generic thumb rule are quite straightforward, both in theory and practice. A general trend with respect to the top ranked happy and peaceful countries is that all these nations have a sense of community and shared responsibility (although immigrant inclusivity, social diversity, and race and ethnic heterogeneity might be questionable in some of the Nordic countries) and thus are much more peaceful, happier, healthier, and overall prosperous. Canada, for instance, is the only country in the Americas to make it to the top ten in both health and peace indices, respectively. Perhaps, the biggest contributing factor is Canada’s ‘multiculturalism’ (Source: Brosseau L, Dewing M. Canadian Multiculturalism. (2009):32.) – officially adopted by the government during the 1970s and 1980s. Based on these insights, it can very well be argued that a Canadian dream and/or a Nordic dream (not only in terms of economic migration but all other relative factors that determine the quality of life and standard of living) seems far more rewarding than an American dream in order to pursue a happier and fulfilling life in every sense of the word. However, this beyond the scope of this article!
Conclusion and Way Forward
In conclusion, the way forward to ensure and sustain good health, overall well-being, greater internal and external peace, enhanced socioeconomic prosperity, and universal happiness is to replace the vicious cycle of violence (of all forms) and poor health outcomes with the virtuous cycle of higher levels of peace, prosperity, and health. This can be made possible only if the world transitions towards the idea of sustainable and ‘balanced’ abundance – an intricate balance between excess and deficiency, as noted by Aristotle almost two millennia ago and Mahatma Gandhi a century ago (Source: Dalton D. Mahatma Gandhi: Nonviolent Power in Action. Columbia University Press; 2012. 353 p.). The path to stable and sustainable prosperity requires the non-tangible and dynamic concept of happiness to be embedded in all policies, inherent at all governance levels, and amongst all individuals to transition towards a healthier and peaceful world in the future.
The United Nations (UN) defines violence against women and girls (VAW) as “any act of gender-based violence that results in, or is likely to result in, physical, sexual, or mental harm or suffering to women, including threats of such acts, coercion or arbitrary deprivation of liberty, whether occurring in public or in private life”. Globally, one in three women experience physical and/or sexual violence by a partner or sexual violence by a non-partner. The most extreme form of VAW on a continuum of violence and discrimination against women and girls is the intentional killing of women called ‘femicide’.
The term ‘femicide’ encompasses femicide perpetrated by men (current or former intimate partners); female-perpetrated femicide; and femicide involving family members as well. Femicide constitutes an ongoing abuse in the home, threats or intimidation, sexual violence and/or situations where gender power imbalances arise out of resource disparities such as lower levels of education and income as well as women’s low social and economic status. VAW is a major global public health concern and femicide, specifically, is a complex issue as aforementioned femicide categories are not always distinct and quite often overlap.
Femicide – A Global Epidemic
Femicide is a critical public health issue and the prevalence of femicide transcends geographic boundaries. The causes and consequences of femicide are an interplay of a myriad of social, economic, political, and cultural factors. One third of global femicide cases are reported to be committed by an intimate partner, with femicide rates ranging from 3.1 victims per 100,000 females in Africa, 1.6 in the Americas, 1.3 in Oceania, 0.9 in Asia and 0.7 in Europe.
In the United States, for instance, pregnant women are at an increased risk of intimate partner femicide. Evidence from the United Kingdom suggests that femicide has a ‘collateral’ consequence – murder of children, witnesses, and perceived allies, including lawyers, relatives, family friends, and neighbours.
Further, the issue of missing and murderedIndigenous women and girls in Canada has received much national and international attention. Although most of such femicides could be categorized as intimate partner femicide, there is more to it than meets the eye. It is pertinent to understand the ‘intersectional’ element of such femicides – the combined role of intersecting identities of ‘Indigenous’ and ‘woman’ that might be leading to a higher risk factor in such femicides. Furthermore, Europe (Source: van Eck, C. (2003). Purified by blood: honour killings amongst Turks in the Netherlands. Amsterdam: Amsterdam University Press.), Australia, North America, and much of the Western countries (Source: Gill A.K., Strange C., & Roberts K.A. (Eds.). (2014). “Honour” killing and violence: theory, policy and practice. Basingstoke, Hampshire: Palgrave Macmillan) are experiencing a surge in the number of femicide cases, specifically related to the killing of females in the name of ‘honour’.
‘Honour’ and ‘Dowry’ related femicides – A Sociocultural Issue
‘Honour’-related femicide is usually addressed as ‘honour killing’ which involves “ the murder of a girl or woman resulting from an actual or assumed sexual or behavioural transgression (adultery, sexual intercourse, pregnancy outside marriage, or even for being raped)”. This type of femicide is often seen to protect family reputation and to follow patriarchal and age-old religious traditions or cultural beliefs. The UN estimates that approximately 5,000 women and girls are murdered each year in ‘honour killings’ by members of their families. Honour killings are widespread across the globe, but are especially common in the Middle East and South Asia.
Further, with respect to dowry-related femicides, despite laws in place, dowry-related disputes and deaths are still commonplace, especially in India. In 2018 alone, about 7,000 women (brides) were killed for dowry-related disputes. These ‘bride killings’ occur around wedding time or during the initial years of the marriage, resulting from constant threats (disputes continuing for years) from the groom’s family, and torture (verbal abuse and/or physical harassment) in order to get a larger dowry. Such incidents include ‘bride burning’ (a form of domestic violence and usually reported as ‘kitchen accidents’) in which the bride ends up being burned to death.
Ending Global Femicide
The global sociocultural menace of VAW and femicides needs to be addressed via stringent legislations (including enhanced surveillance, universal screening, and reporting of intimate partner violence and femicides) and devising global response systems (sensitization of police, media, social workers and healthcare professionals in the developing world as well as developed countries). That is, applying country-specific and culture-specific socio-ecological model (SEM) remedies in order to address this grave issue, holistically. SEM response must strive to address the upstream causes and downstream consequences associated with femicides occurring at individual, family, community and wider society levels (including system and policy/environmental levels).
Conclusion
VAW and femicide have enormous adverse effects throughout global society. No cultural, social, or religious belief is above fundamental human rights. VAW and femicide is an attack on women’s human rights and threatens to devalue the worth of women and treat them as less than human. The world needs to collectively address femicide and end such horrific acts of violence emanating from fragile masculine morality, resulting in targeted elimination of women. Femicide cannot become second nature to the current global culture. This can only be made possible when each one of us acknowledges the dignity of women and girls and the value of their very existence.
This blog post was originally published in the University of Toronto's Global Health Magazine - Juxtaposition on December 18th, 2019.
It is 2022, that is, two years into the COVID-19 pandemic. The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus’s deadly effects appear to be waning globally. Based on the factors such as global case rate, positivity rate, daily death count, virus reproduction rate, susceptibility of the population, social behavior changes (masking, vaccinations, among others), pathogen transitionality, etc., COVID-19 is slowly starting to plummet globally with some nations still experiencing high caseloads due to the much transmissible (compared to the Delta variant) Omicron variant. Currently, the nature of next phase of the pandemic is what is being hotly debated in the scientific community and outside. Is the pandemic about to get over? Are we in the process of transitioning from a pandemic phase to an endemic phase? What would endemicity phase entail? What are other probable future scenarios that could affect public health response to the pandemic? These are some of the questions that would constitute the deliberations in this article.
Defining Endemicity
What does endemicity actually mean? Epidemic means ‘upon the people’ (epi+demos) and endemic means ‘within the people’ (en+demos). An endemic disease is one that becomes potentially stabilized within a population – not vanishing completely but present with symptoms that could be categorized as mild or harmless or even with low transmissibility. This does not mean that global COVID outbreaks would not occur. That said, it is difficult to predict for sure regarding the next phase of the pandemic. After a global Omicron variant surge registering elevated level of COVID-19 cases, the evolving coronavirus seems to be finally transitioning from a pandemic to an endemic phase. An endemic phase could observe lifting of country-specific COVID-19 pandemic-related travel restrictions, mask and testing mandates, among other restrictions. This does not mean that public should confuse COVID-19 with influenza. Thus, the global community needs to be cautious as ever – aware that we might be entering an endemic phase, however, cognizant of the fact that we need to be well prepared of the difficult days ahead! In other words, we need to be extra vigilant during this crucial juncture wherein the world is at the crossroads of overturning this hopefully once-in-a-century global public health crisis. The evolutionary and transitional nature of the coronavirus is what makes it inherently unpredictable to counter completely worldwide. Different national healthcare system approaches and capacities, seasonality, and unfavorable geographic location/distribution would allow more variants to spread successfully. This in turn could lead to prolonged emergency situation with new waves of epidemics cropping up in distinct parts of the world. One risky factor that is emerging is the spread of Omicron subvariant – BA.2. Thus, it might be useful to start thinking about a global endemic resolution strategy for the purposes of COVID-19 pandemic preparedness rather than becoming a casualty of an ‘endemic delusion‘.
Evolution of COVID-19 – A ‘new normal‘
As discussed above, one likely evolutionary scenario for the future of SARS-CoV-2 is endemicity. Humans currently coexist with four known endemic coronaviruses. Their scientific designations, that is, 229E (llama coronavirus), OC43 (bovine coronavirus), NL63 (NetherLand 63), and HKU1 (Hong Kong University 1) are known as common cold coronaviruses. The immunity to these coronaviruses’ wanes with time. Thus, infections can recur throughout the human lifespan. This is the most likely scenario for COVID-19 pandemic within the realm of possibilities. Additionally, some non-mutually exclusive evolutionary scenarios are contemplated in the next sections of this article.
Modified diseasesand symptoms
A likely scenario could be a mutant virus producing an altogether different (altered) disease and symptoms. In this scenario, the SARS-CoV-2 could infect new cells in the human body. That is, the coronavirus could infect and affect other organ systems rather than predominantly infecting and affecting the respiratory system only. The ultimate effect on the human body is difficult to predict as it depends on the severity of organ(s) damaged – intestine, kidney, and the central nervous system.
Recombinant coronavirus
Current evidence suggests that there is a likelihood that SARS-CoV-2 evolves into a novel hybrid – combination of genetic material of the human SARS-CoV-2 and the genetic material of an existing animal coronavirus. Given the huge caseloads of SARS-CoV-2 infected humans, there is a good probability that someone somewhere on this planet might be simultaneously infected with SARS-CoV-2 and an animal coronavirus. SARS-CoV-2-infected humans who have close contact with coronavirus-infected animals could serve as hosts for the novel recombinant viruses. Regardless of where and how novel hybrid variations of coronavirus might arise, the recombinant virus could easily diminish SARS-CoV-2 immunity and could even have different disease genetics than what has been observed in context of COVID-19 and its variants.
Exploitation of human immune response
There is likelihood that the future scenario could entail a variant that exploits human immune response. The major variants of SARS-CoV-2 virus such as Alpha through Omicron (and now reportedly Deltacron) led to virus evolution that helped evade the human immune system. Further, there is a possibility of exploitation of the immune system. For instance, when humans are infected with dengue (not a coronavirus), the immune system produces an immune response entailing illness with high fever and muscle and joint pain. The initial immune response to dengue makes the individual immune to future exposures with that same type of dengue virus. However, if the person gets a reinfection from dengue-type virus, the initial infection increases the severity of disease(s) instead of providing protection against it. This is due to an effect called ‘antibody-dependent enhancement‘ (ADE) of virus infection and disease. This is worrisome because SARS-CoV-2 may evolve to use ADE to increase virus growth and transmission, and a new or hybrid variant could explosively spread through immune populations across the globe.
Conclusion
All of the above listed future scenarios are equally likely, however, my hunch is that SARS-CoV-2 will enter a phase of endemicity in the months to come. That said, other scenarios discussed in this article are within the realm of possibility – altered disease, recombinant viruses, and/or exploitation of immune response. Some other scenarios (not discussed in this article) that might take place is infection transmission from humans to animals and spillover effects of reinfection from animals back to humans. Further, there could be a situation where there is an uptick of transmissibility from chronically infected people with ‘long Covid‘ to immune populations. All these scenarios could decide how the COVID-19 pandemic end game will play out. A new coronavirus variant could emerge anywhere in the world and spread like wildfire in a matter of few weeks as has been the case with successive variations of the evolving coronavirus. The hope is that COVID-19 would recede rather than intensify from the current scenario.
In closing, we are about to reach there but we are not quite there yet. This translates to public health policy measures to be centered around masks and vaccines (including booster shots to counter variants). Therefore, the pandemic end game still seems like a waiting game! It remains to be seen which way the wind blows.
Malnutrition is an inter-generational phenomenon. The vicious cycle of malnutrition leads to health crisis and is no less than an epidemic.
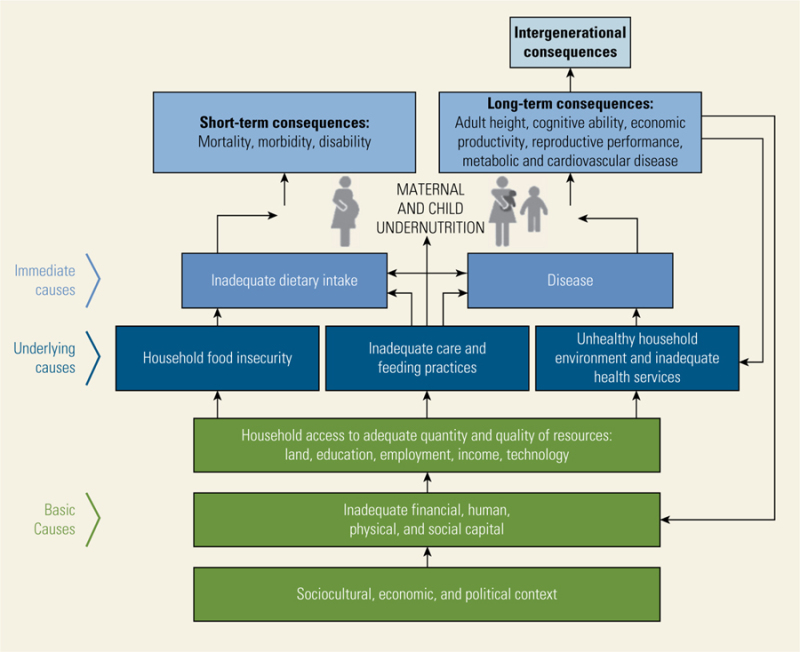
Malnutrition refers to deficiencies, excesses or imbalances in a person’s intake of energy and/or nutrients. The term malnutrition encompasses two broad categories of conditions, that is, ‘undernutrition’ including stunting (low height-for-age), wasting (low weight-for-height), and underweight (low weight-for-age), and micronutrient deficiency or insufficiency (lack of important vitamins and minerals); and ‘overnutrition’ encapsulating malnourishment caused due to consuming too many calories leading to overweight/obesity (WHO, 2016). Malnutrition issue is multidimensional and multisectoral in nature. Undernourished individuals can no longer maintain natural bodily capacities, such as growth, immunity, intellectual and physical capacities, and pregnancy and lactation in women (UNICEF, 2006).
Although malnutrition can manifest in multiple ways, the pathways to prevention involves adequate maternal nutrition, optimal breastfeeding practices, access to and affordability of nutritious food for early childhood development, and a healthy environment including access to basic healthcare services and opportunities for physical activity. Combating all forms of malnutrition is one of the greatest public health challenges, in India and the world.
Undernutrition in India
The Ministry of Health and Family Welfare, Government of India, released the National Health Policy in the year 2017, which highlighted the negative impact of malnutrition on the population’s productivity, and its contribution to higher morbidity and mortality. Although India has witnessed significant progress in its battle against malnutrition over the past several years, the progress has been quite uneven, and child malnutrition rates remain high in many parts of the country.
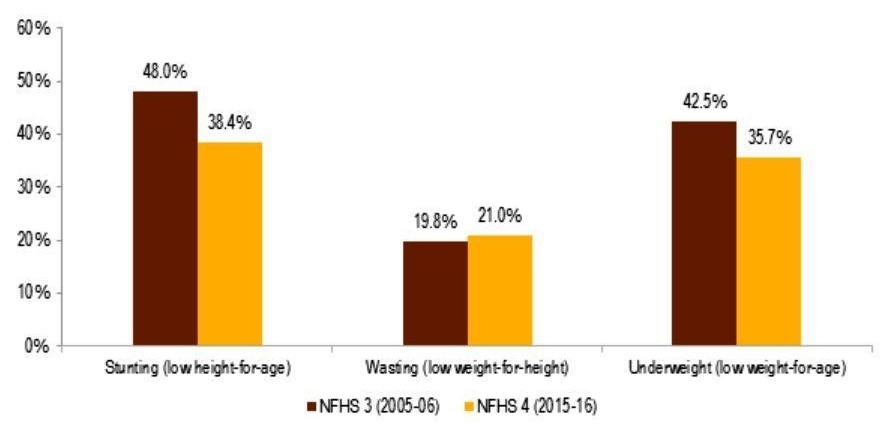
According to the National Family Health Survey (2015-16), the proportion of underweight children fell nearly 7 percent to 36 percent, while the proportion of stunted children declined nearly 10 percent to 38 percent. Despite the progress, these rates are still considerably higher than those of many low- and middle-income countries in sub-Saharan Africa.
Comparative analysis of undernutrition levels in India (National Family Health Survey 3 & 4)
Empirical evidence suggests that socioeconomic factors such as low income, poverty, food insecurity, maternal illiteracy, low societal status of women, poor sanitation and hygiene, and other environmental and structural factors are likely reasons for high malnutrition in India.
The multidimensional health inequities and social determinants of malnutrition have been elucidated in the subsequent sections of this article.
Social Determinants of Malnutrition – Empirical Evidence
There is considerable empirical evidence that has recognized the importance of social determinants of health (SDOH) in India. Cowling et al. (2014) extracted household and individual-level SDOH indicators from national household surveys conducted between 1990 and 2011. The study indicated air pollution, child undernutrition, unimproved sanitation, employment conditions, and gender inequality as priority SDOH issues in India. This finding is critical as the aforementioned factors have direct and/or indirect implications for malnutrition in India.
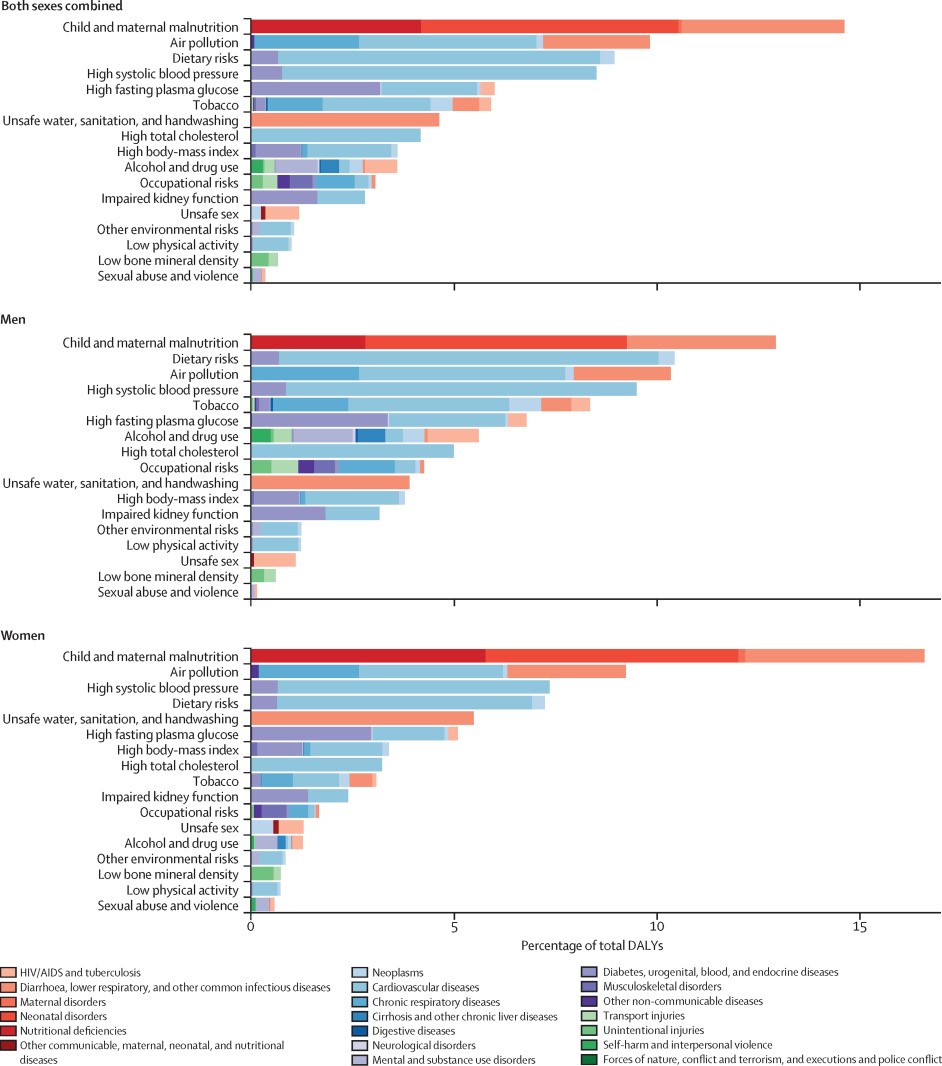
Further, the Global Burden of Disease Study estimated disease burden and risk factors to effectively improve population health in India over time. The report concluded that maternal and child malnutrition were among the leading risk factors accounting for 15% of the total disability-adjusted life-years (DALYs). The study also noted that child and maternal malnutrition and unsafe water, sanitation, and hand washing contributed more to the DALYs in women than in men. Conversely, the proportion of total DALYs due to dietary risks, high systolic blood pressure, high fasting plasma glucose, high cholesterol, and high body-mass index were found to be highest in the states that experienced high epidemiological transition level. This, in essence, explains the reason behind the co-existence of underweight and overweight, symptomatic of the ‘double burden of malnutrition‘ (DBM) in India.
DALYs attributable to risk factors in India (2016)
Furthermore, a research study by Corsi et al. (2016) assessed the simultaneous contribution of 15 known risk factors for child chronic undernutrition in India. The study concluded that maternal stature, education, household wealth, dietary diversity, and maternal body mass index (BMI) were the top five risk factors, accounting for more than 65% of the Population Attributable Risks for child undernutrition.
Similar findings were reported by Kim et al. (2017) after assessing the relative importance of 13 risk factors such as complementary feeding, breastfeeding, feeding frequency, dietary diversity, maternal height, BMI, education, age at marriage, child vaccination, access to improved drinking source and sanitation facilities, household indoor air quality, and household wealth. India was found to have the highest prevalence of child stunting due to short maternal stature, lack of nutrition supplementation, among others.
The above research findings point towards the complex, non-linear, multi-factorial nature and scope (interplay of child, maternal, household, environmental, and socioeconomic factors) of malnutrition. Thus, it is critical to understand the multidimensional social and biological mechanisms that have resulted in abysmal child and maternal nutritional profile in India. Each of these factors has been examined in detail in the following section of this article.
Pathways to Malnutrition: Social and Biological Factors
The key social factors responsible for high malnutrition in India pertain to the socioeconomic status and inequalities, women’s status and empowerment, gender disparities, adult (maternal) literacy, environmental determinants, structural barriers, among others.
Socioeconomic Status (SES)
There is a general notion that economic growth reduces malnutrition. However, in India, evidence suggests that macroeconomic growth is not correlated with any substantial reductions in the prevalence rates of malnutrition over time.
An assessment of trends in social disparities and childhood undernutrition by Subramanyam et al. (2010, 2011) noted that the socioeconomic disparities either increased or remained constant during a time of major economic growth. The positive effect of economic growth experienced by children from socioeconomically privileged households, with better educated mothers was found to be greater than disadvantaged children. Kumar et al. (2015) examined the patterns in socioeconomic inequality in urban India and noted a decline in the prevalence of childhood undernutrition to be higher among the affluent socioeconomic groups than among the worse-off groups. Similarly, Bharati et al. (2011) found that children with illiterate mothers, of lower age groups, or from low standard of living households are more prone to become malnourished.
Interestingly, SES also has adverse effects on the rising DBM issue in India, as reported by Gaur et al. (2013) that examined the intra-city distribution of women’s nutritional profile with a focus on slum and non-slum divide. The study found that there was a prevalence of undernutrition among slum dwellers and overnutrition among non-slum women.
Further, there is evidence linking social class and nutritional stress. Mandal et al. (2011) found a direct relationship between the social class and nutritional outcomes, that is, children belonging to lower social group were found to have lower body fat. This pattern of socioeconomic segregation is consistent with the fact that there is a larger concentration of underweight women among the low socioeconomic group and of overweight/obese women among the high socioeconomic group (Kulkarni et al. 2017). Additionally, there are other socioeconomic perspectives such as food price shocks, household income, and resource allocation that have adverse effects on dietary quality and nutritional status (Bouis et al., 2011; Borkotoky et al., 2018).
Economic prosperity alone is unlikely to reduce the burden of malnutrition in India. Addressing the broader SDOH that negatively contributes to malnutrition prevalence, especially in specific demographic subgroups such as rural young females, as identified by Siddiqui et al. (2017), is pertinent in curbing high malnutrition rates in India. This might require health policies and programs with staggered approach focusing on such lower SES populations.
Gender Disparity
In India, gender differential in the nutritional status is prevalent at all levels of income and follow a social gradient: the lower the SES, the worse the nutritional profile.
Mandal et al. (2011) explained an implicit issue of gender disparity plaguing the malnutrition issue in India. The study reported inadequate nutrition received by girl child belonging to the lower social stratum and thus a lower body fat. Among the marginalized populations like Indian tribes, women, in particular, are the worst sufferers of nutritional stress (Kshatriya & Acharya, 2016).
There have been found to be persistent gendered effects of siblings on child malnutrition for both boys and girls. Raj et al. (2015) documented that having brothers heightens girl (sisters’) risk for acute malnutrition (wasting), whereas having multiple sisters increases girl’ risk for chronic malnutrition (stunting/underweight). However, malnutrition among boys was found to be less affected by the gender of siblings.
Women’s Social Status and Empowerment
Closely linked with gender disparity is the issue of low status of women in Indian society, which hinders equitable access to nutrition. There is evidence linking higher women’ and/or maternal status within a community with positive effects on daughter’s nutritional status. Bose (2011) investigated whether differences in women’s social status, both at the individual and community levels, can explain the differential in nutritional allocation among children. The study concluded that girl child is less likely than the boy child to receive supplemental food and thus more likely to be malnourished.
Further, there is a direct positive relationship between maternal autonomy (indicated by financial and physical autonomy) and childcare. Women with higher autonomy are significantly less likely to have a stunted child (Shroff et al., 2009).
Thus, lower levels of women empowerment in India has critical ramifications leading to inter-generational cycle of malnutrition.
Sociocultural Factors
As discussed in previous sections of this article, there are a myriad of social factors that play a critical role in impacting the biological aspects with inter-generational and multi-generational effects on malnutrition. Sociocultural factors such as child marriage (a ritual still largely prevalent in backward rural areas of the country) have strong associations with morbidity and mortality of infants and children under the age of 5 in India. The risk of malnutrition is higher in young children born to mothers married as minors than among those born to women married at a majority age (Raj et al., 2010).
Further, inequitable nutritional allocation in early life for girls also has a direct negative impact on adolescent undernutrition due to sub-optimal childhood nutrition levels. Chronic undernutrition and prevailing sociocultural conditions also result in adverse adolescent pregnancy outcomes and impede post-menarcheal height growth (Rao et al., 2010). This phenomenon translates to higher child stunting rates in India.
Furthermore, domestic violence is also considered to be a major cause of malnutrition due to detrimental effects on women’s physical and psychological health. As noted by Ackerson & Subramanian (2008), the possible mechanisms for this relation include withholding of food as a form of abuse and stress-mediated influences of domestic violence on nutritional outcomes.
Environmental Factors
Malnutrition and availability of potable water and proper sanitation facilities are integral and interrelated components. As discussed earlier, although over the past decade, India’s economic growth has been remarkable – yet almost half of India’s children under the age of 5 remain stunted.
Indian children suffer from malnutrition due to recurring gastrointestinal infections (resulting from lack of sanitation rather than food insecurity). High number of diarrhoeal infections, lack of personal hygiene practices, and poor health and sanitation infrastructure further exacerbate the issue of chronic malnutrition among children (Saxton et al., 2016).
Potential of Public Nutrition Schemes
Child and maternal malnutrition continues to be the leading risk factor in India. The high present and future disease burden caused by malnutrition in women of reproductive age, pregnancy, and children under the age of 5 have led to interventions focused predominantly on these population subgroups.
In order to mitigate malnutrition and meet the United Nations Sustainable Development Goals targets by 2030, India has adopted the Newborn Action Plan focusing on 187 priority districts. Further, the Government of India program – Integrated Child Development Services, launched in 1975, has the goal to provide supplementary nutrition and health education, and other preschool childhood development services across the country. The Mid Day Meal Scheme, launched in 1995, provides free lunch to school children. The Indian Government legislated the National Food Security Act in 2013, with the objective of providing food and nutritional security through provision of subsidized food grains and focused nutritional support to women and children. The Rural Sanitation Program initially launched in 1986, and the revamped version – ‘Clean India Mission’, launched in 2014 by the current Prime Minister of India has an overarching goal to clean India and eliminate open defecation.
Despite a major focus of public health programs to address malnutrition in India for several decades now, the current trend seems to be persistent with rising anemia and DBM. Critical gaps in the current public health and social welfare schemes point towards a myopic view of the malnutrition issue. Until recently, the health interventions have largely focused on nutrition-specific interventions (like Mid-Day Meal, among others) leading to under-investments in behaviour change and nutrition-sensitive interventions. This has further led to a suboptimal level of integration of vital upstream factors and social determinants of health, including girls’ education, nutritional awareness, hygiene behaviour, family planning practices, social assistance programs, and other structural factors, in order to holistically address the problem of malnutrition in India.
Conclusion and Way Forward
This article presented evidence of the multidimensional and multi-generational nature of health inequities and social determinants of health associated with malnutrition in India.
Subramanian & Subramanyam (2015) and Joe et al. (2016) noted that a ‘support‐led’ strategy rather than simply relying on a ‘growth‐mediated’ strategy for addressing the root causes of malnutrition is the need of the hour. Going forward, there is an urgent need to combat all forms of malnutrition via nutrition-sensitive, health promotion, and social behaviour change interventions in conjunction with improvement of socioeconomic and human development indicators via provision of better nutrition, potable water, and proper sanitation for higher, positive, and tangible impact among the most vulnerable sections of the society. That said, existing public nutrition schemes in India are suboptimal; plagued with pilferage; inconstant beneficiary targeting; and poor implementation. This needs to be reversed via plugging leakages in public nutrition schemes (both in-kind and direct cash transfers) and addressing current impediments in social assistance schemes by improving beneficiary identification and targeting, that is, efficiently connecting hard-to-reach and chronically malnourished populations, especially mothers and children, with robust nutrition-related interventions.
References
Ackerson, L. K., & Subramanian, S. V. (2008). Domestic violence and chronic malnutrition among women and children in india. American Journal of Epidemiology, 167(10), 1188-1196.
Bharati, S., Pal, M., Chakrabarty, S., & Bharati, P. (2011). Trends in socioeconomic and nutritional status of children younger than 6 years in india. Asia-Pacific Journal of Public Health, 23(3), 324-340.
Borkotoky, K., Unisa, S., & Gupta, A. K. (2018). State-level dietary diversity as a contextual determinant of nutritional status of children in india: A multilevel approach. Journal of Biosocial Science, 50(1), 26-52.
Bose, S. (2011). The effect of women’s status and community on the gender differential in children’s nutrition in india. Journal of Biosocial Science, 43(5), 513-533.
Bouis, H. E., Eozenou, P., & Rahman, A. (2011). Food prices, household income, and resource allocation: Socioeconomic perspectives on their effects on dietary quality and nutritional status. Food & Nutrition Bulletin, 32(1 Suppl), S14-23.
Corsi, D. J., Mejia-Guevara, I., & Subramanian, S. V. (2016). Risk factors for chronic undernutrition among children in india: Estimating relative importance, population attributable risk and fractions. Social Science & Medicine, 157, 165-185.
Cowling, K., Dandona, R., & Dandona, L. (2014). Social determinants of health in india: Progress and inequities across states. International Journal for Equity in Health, 13, 88.
Gaur, K., Keshri, K., & Joe, W. (2013). Does living in slums or non-slums influence women’s nutritional status? evidence from indian mega-cities. Social Science & Medicine, 77, 137-146.
India State-Level Disease Burden Initiative Collaborators. (2017). Nations within a nation: Variations in epidemiological transition across the states of india, 1990-2016 in the global burden of disease study. Lancet, 390(10111), 2437-2460.
Joe, W., Rajaram, R., & Subramanian, S. V. (2016). Understanding the null-to-small association between increased macroeconomic growth and reducing child undernutrition in india: Role of development expenditures and poverty alleviation. Maternal & Child Nutrition, 12(Suppl 1), 196-209.
Kim, R., Mejia-Guevara, I., Corsi, D. J., Aguayo, V. M., & Subramanian, S. V. (2017). Relative importance of 13 correlates of child stunting in south asia: Insights from nationally representative data from afghanistan, bangladesh, india, nepal, and pakistan. Social Science & Medicine, 187, 144-154.
Kshatriya, G. K., & Acharya, S. K. (2016). Triple burden of obesity, undernutrition, and cardiovascular disease risk among indian tribes. PLoS ONE [Electronic Resource], 11(1), e0147934.
Kulkarni, V. S., Kulkarni, V. S., & Gaiha, R. (2017). “Double burden of malnutrition”: Reexamining the coexistence of undernutrition and overweight among women in india. International Journal of Health Services, 47(1), 108-133.
Kumar, A., Kumari, D., & Singh, A. (2015). Increasing socioeconomic inequality in childhood undernutrition in urban india: Trends between 1992-93, 1998-99 and 2005-06. Health Policy & Planning, 30(8), 1003-1016.
Mandal, G. C., Bose, K., & Koziel, S. (2011). Impact of social class on body fatness among rural pre-school bengalee hindu children of arambagh, west bengal, india. Homo, 62(3), 228-236.
Mandal, G. C., Bose, K., & Koziel, S. (2011). Impact of social class on body fatness among rural pre-school bengalee hindu children of arambagh, west bengal, india. Homo, 62(3), 228-236.
Ministry of Consumer Affairs Food and Public Distribution, Government of India (2013). National Food Security Act (NFSA). Retrieved from http://dfpd.nic.in/public-distribution.htm
Press Information Bureau, Ministry of Rural Development, Government of India (2014, September 25). Government to spend about 2 lakh crore rupees for Swachh Bharat mission more than 11 crore toilets will be built in 5 years. Retrieved from http://pib.nic.in/newsite/PrintRelease.aspx?relid=110036
Raj, A., McDougal, L. P., & Silverman, J. G. (2015). Gendered effects of siblings on child malnutrition in south asia: Cross-sectional analysis of demographic and health surveys from bangladesh, india, and nepal. Maternal & Child Health Journal, 19(1), 217-226.
Raj, A., Saggurti, N., Winter, M., Labonte, A., Decker, M. R., Balaiah, D., & Silverman, J. G. (2010). The effect of maternal child marriage on morbidity and mortality of children under 5 in india: Cross sectional study of a nationally representative sample. Bmj, 340, b4258.
Rao, S., Gokhale, M., Joshi, S., & Kanade, A. (2010). Early life undernutrition and adolescent pregnancy outcome in rural india. Annals of Human Biology, 37(4), 475-487.
Saxton, J., Rath, S., Nair, N., Gope, R., Mahapatra, R., Tripathy, P., & Prost, A. (2016). Handwashing, sanitation and family planning practices are the strongest underlying determinants of child stunting in rural indigenous communities of jharkhand and odisha, eastern india: A cross-sectional study. Maternal & Child Nutrition, 12(4), 869-884.
Shroff, M., Griffiths, P., Adair, L., Suchindran, C., & Bentley, M. (2009). Maternal autonomy is inversely related to child stunting in andhra pradesh, india. Maternal & Child Nutrition, 5(1), 64-74.
Siddiqui, M. Z., & Donato, R. (2017). Undernutrition among adults in india: The significance of individual-level and contextual factors impacting on the likelihood of underweight across sub-populations. Public Health Nutrition, 20(1), 130-141.
Subramanian, S. V., & Subramanyam, M. A. (2015). Limits to economic growth: Why direct investments are needed to address child undernutrition in india. Journal of Korean Medical Science, 30(Suppl 2), S131-3.
Subramanyam, M. A., Kawachi, I., Berkman, L. F., & Subramanian, S. V. (2010). Socioeconomic inequalities in childhood undernutrition in india: Analyzing trends between 1992 and 2005. PLoS ONE [Electronic Resource], 5(6), e11392.
Subramanyam, M. A., Kawachi, I., Berkman, L. F., & Subramanian, S. V. (2011). Is economic growth associated with reduction in child undernutrition in india?. PLoS Medicine / Public Library of Science, 8(3), e1000424.